

Long-term risks of respiratory diseases in patients infected with SARS-CoV-2: a longitudinal, population-based cohort study
- PMID: 38389713
- PMCID: PMC10882104
- DOI: 10.1016/j.eclinm.2024.102500
Long-term risks of respiratory diseases in patients infected with SARS-CoV-2: a longitudinal, population-based cohort study
Abstract
Background: In the post-pandemic era, growing apprehension exists regarding the potential sequelae of COVID-19. However, the risks of respiratory diseases following SARS-CoV-2 infection have not been comprehensively understood. This study aimed to investigate whether COVID-19 increases the long-term risk of respiratory illness in patients with COVID-19.
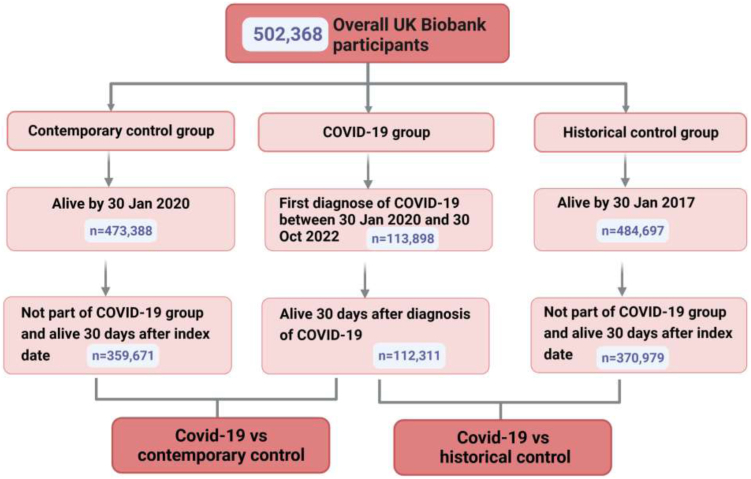
Methods: In this longitudinal, population-based cohort study, we built three distinct cohorts age 37-73 years using the UK Biobank database; a COVID-19 group diagnosed in medical records between January 30th, 2020 and October 30th, 2022, and two control groups, a contemporary control group and a historical control group, with cutoff dates of October 30th, 2022 and October 30th, 2019, respectively. The follow-up period of all three groups was 2.7 years (the median (IQR) follow-up time was 0.8 years). Respiratory outcomes diagnosed in medical records included common chronic pulmonary diseases (asthma, bronchiectasis, chronic obstructive pulmonary disease (COPD), interstitial lung disease (ILD), pulmonary vascular disease (PVD), and lung cancer. For the data analysis, we calculated hazard ratios (HRs) along with their 95% CIs using Cox regression models, following the application of inverse probability weights (IPTW).
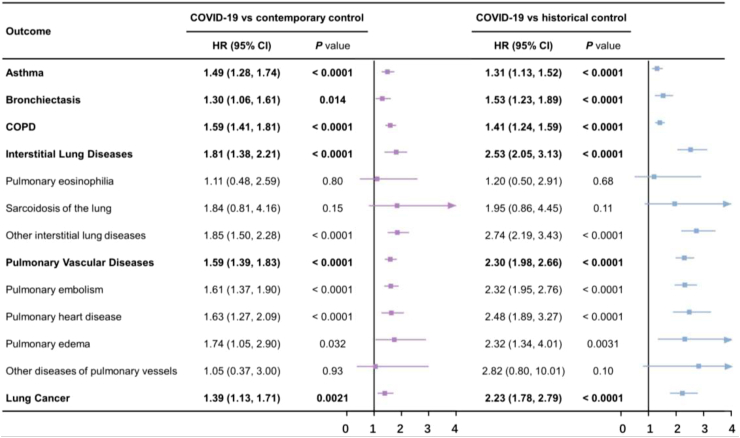
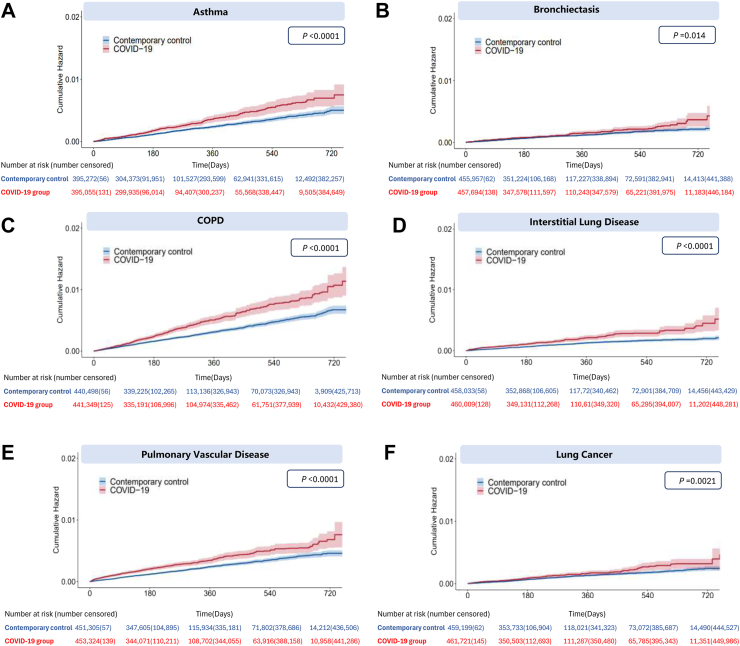
Findings: A total of 3 cohorts were included in this study; 112,311 individuals in the COVID-19 group with a mean age (±SDs) of 56.2 (8.1) years, 359,671 in the contemporary control group, and 370,979 in the historical control group. Compared with the contemporary control group, those infected with SARS-CoV-2 exhibited elevated risks for developing respiratory diseases. This includes asthma, with a HR of 1.49 and a 95% CI 1.28-1.74; bronchiectasis (1.30; 1.06-1.61); COPD (1.59; 1.41-1.81); ILD (1.81; 1.38-2.21); PVD (1.59; 1.39-1.82); and lung cancer (1.39; 1.13-1.71). With the severity of the acute phase of COVID-19, the risk of pre-described respiratory outcomes increases progressively. Besides, during the 24-months follow-up, we observed an increasing trend in the risks of asthma and bronchiectasis over time. Additionally, the HR of lung cancer for 0-6 month follow-up was 3.07 (CI 1.73-5.44), and the association of lung cancer with COVID-19 disease disappeared at 6-12 month follow-up (1.06; 0.43-2.64) and at 12-24 months (1.02; 0.45-2.34). Compared to those with one SARS-CoV-2 infection, reinfected patients were at a higher risk of asthma (3.0; 1.32-6.84), COPD (3.07; 1.42-6.65), ILD (3.61; 1.11-11.8), and lung cancer (3.20; 1.59-6.45). Similar findings were noted when comparing with a historical cohort serving as a control group, including asthma (1.31; 1.13-1.52); bronchiectasis (1.53; 1.23-1.89); COPD (1.41; 1.24-1.59); ILD (2.53; 2.05-3.13); PVD (2.30; 1.98-2.66); and lung cancer (2.23; 1.78-2.79).
Interpretation: Our research suggests that patients with COVID-19 may have an increased risk of developing respiratory diseases, and the risk increases with the severity of infection and reinfection. Even during the 24-month follow-up, the risk of asthma and bronchiectasis continued to increase. Hence, implementing appropriate follow-up strategies for these individuals is crucial to monitor and manage potential long-term respiratory health issues. Additionally, the increased risk in lung cancer in the COVID-19 individuals was probably due to the diagnostic tests conducted and incidental diagnoses.
Funding: The National Natural Science Foundation of China of China Regional Innovation and Development Joint Foundation; National Natural Science Foundation of China; Program for High-level Foreign Expert Introduction of China; Natural Science Foundation for Distinguished Young Scholars of Guangdong Province; Guangdong Basic and Applied Basic Research Foundation; Climbing Program of Introduced Talents and High-level Hospital Construction Project of Guangdong Provincial People's Hospital; VA Clinical Merit and ASGE clinical research funds.
Keywords: COVID-19 (coronavirus disease 2019); Epidemiological study; Respiratory diseases; SARS-CoV-2 (severe acute respiratory syndrome coronavirus 2).
© 2024 The Author(s).
Conflict of interest statement
All authors declare no competing interests.
Figures
Similar articles
-
Associations of proton pump inhibitors with susceptibility to influenza, pneumonia, and COVID-19: Evidence from a large population-based cohort study.Elife. 2024 Jul 16;13:RP94973. doi: 10.7554/eLife.94973. Elife. 2024. PMID: 39012339 Free PMC article.
-
Risks of digestive diseases in long COVID: evidence from a population-based cohort study.BMC Med. 2024 Jan 10;22(1):14. doi: 10.1186/s12916-023-03236-4. BMC Med. 2024. PMID: 38195495 Free PMC article.
-
Mortality and Morbidity Effects of Long-Term Exposure to Low-Level PM2.5, BC, NO2, and O3: An Analysis of European Cohorts in the ELAPSE Project.Res Rep Health Eff Inst. 2021 Sep;2021(208):1-127. Res Rep Health Eff Inst. 2021. PMID: 36106702 Free PMC article.
-
Universal screening for SARS-CoV-2 infection: a rapid review.Cochrane Database Syst Rev. 2020 Sep 15;9(9):CD013718. doi: 10.1002/14651858.CD013718. Cochrane Database Syst Rev. 2020. PMID: 33502003 Free PMC article.
-
UK Electronic Healthcare Records for Research: A Scientometric Analysis of Respiratory, Cardiovascular, and COVID-19 Publications.Pragmat Obs Res. 2024 Aug 15;15:151-164. doi: 10.2147/POR.S469973. eCollection 2024. Pragmat Obs Res. 2024. PMID: 39161588 Free PMC article. Review.
Cited by
-
Outpatient utilization trend of bronchodilator and anti-inflammatory agents in the pandemic and beyond.Naunyn Schmiedebergs Arch Pharmacol. 2025 Apr 8. doi: 10.1007/s00210-025-04099-7. Online ahead of print. Naunyn Schmiedebergs Arch Pharmacol. 2025. PMID: 40198400
-
Location, Location, Location: Spatial Immune-Stroma Crosstalk Drives Pathogenesis in Asthma.Immunol Rev. 2025 Mar;330(1):e70013. doi: 10.1111/imr.70013. Immunol Rev. 2025. PMID: 39991870 Free PMC article. Review.
-
The Clinical Profile of Pediatric M. pneumoniae Infections in the Context of a New Post-Pandemic Wave.Microorganisms. 2025 May 17;13(5):1152. doi: 10.3390/microorganisms13051152. Microorganisms. 2025. PMID: 40431322 Free PMC article.
-
Nursing and Continuing Care Management Work Plan for People Living With COVID-19: Case Study of the Nakhon Pathom Province.JMIR Nurs. 2025 May 29;8:e65310. doi: 10.2196/65310. JMIR Nurs. 2025. PMID: 40440565 Free PMC article.
-
Towards airway microbiome engineering for improving respiratory health.Adv Drug Deliv Rev. 2025 Aug 6;225:115662. doi: 10.1016/j.addr.2025.115662. Online ahead of print. Adv Drug Deliv Rev. 2025. PMID: 40759399 Review.
References
-
- COVID-19 rapid guideline: managing the long-term effects of COVID-19. National Institute for Health and Care Excellence (NICE); 2020. http://www.ncbi.nlm.nih.gov/books/NBK567261/ - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
