

Effectiveness and cost effectiveness of pharmacological thromboprophylaxis for medical inpatients: decision analysis modelling study
- PMID: 38389721
- PMCID: PMC10882286
- DOI: 10.1136/bmjmed-2022-000408
Effectiveness and cost effectiveness of pharmacological thromboprophylaxis for medical inpatients: decision analysis modelling study
Abstract
Objective: To determine the balance of costs, risks, and benefits for different thromboprophylaxis strategies for medical patients during hospital admission.
Design: Decision analysis modelling study.
Setting: NHS hospitals in England.
Population: Eligible adult medical inpatients, excluding patients in critical care and pregnant women.
Interventions: Pharmacological thromboprophylaxis (low molecular weight heparin) for all medical inpatients, thromboprophylaxis for none, and thromboprophylaxis given to higher risk inpatients according to risk assessment models (Padua, Caprini, IMPROVE, Intermountain, Kucher, Geneva, and Rothberg) previously validated in medical cohorts.
Main outcome measures: Lifetime costs and quality adjusted life years (QALYs). Costs were assessed from the perspective of the NHS and Personal Social Services in England. Other outcomes assessed were incidence and treatment of venous thromboembolism, major bleeds including intracranial haemorrhage, chronic thromboembolic complications, and overall survival.
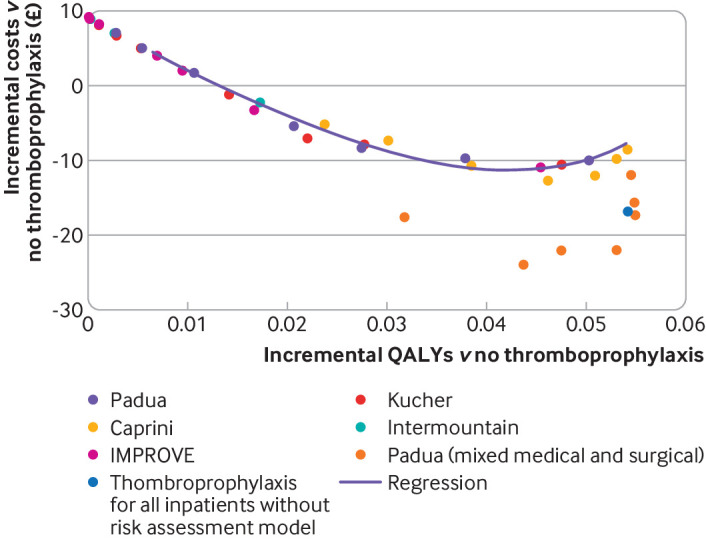
Results: Offering thromboprophylaxis to all medical inpatients had a high probability (>99%) of being the most cost effective strategy (at a threshold of £20 000 (€23 440; $25 270) per QALY) in the probabilistic sensitivity analysis, when applying performance data from the Padua risk assessment model, which was typical of that observed across several risk assessment models in a medical inpatient cohort. Thromboprophylaxis for all medical inpatients was estimated to result in 0.0552 additional QALYs (95% credible interval 0.0209 to 0.1111) while generating cost savings of £28.44 (-£47 to £105) compared with thromboprophylaxis for none. No other risk assessment model was more cost effective than thromboprophylaxis for all medical inpatients when assessed in deterministic analysis. Risk based thromboprophylaxis was found to have a high (76.6%) probability of being the most cost effective strategy only when assuming a risk assessment model with very high sensitivity is available (sensitivity 99.9% and specificity 23.7% v base case sensitivity 49.3% and specificity 73.0%).
Conclusions: Offering pharmacological thromboprophylaxis to all eligible medical inpatients appears to be the most cost effective strategy. To be cost effective, any risk assessment model would need to have a very high sensitivity resulting in widespread thromboprophylaxis in all patients except those at the very lowest risk, who could potentially avoid prophylactic anticoagulation during their hospital stay.
Keywords: Anticoagulants; Economics; Risk management; Thromboembolism.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at http://www.icmje.org/disclosure-of-interest/ and declare: the research described was conducted as part of a wider project funded by the National Institute for Health Research Health Technology Assessment (NIHR HTA) programme; SG is chair of the NIHR Clinical Trials Unit Standing Advisory Committee; KdW reports a grant from Bayer, outside the submitted work; MH has lectured for Pfizer and lectured for and attended a symposium sponsored by Bristol-Myers Squibb Pharmaceuticals; DH is a previous topic expert for National Institute of Health and Care Excellence (NICE) venous thromboembolism guidelines in England; no other relationships or activities that could appear to have influenced the submitted work.
Figures

Similar articles
-
Decision-analysis modeling of effectiveness and cost-effectiveness of pharmacologic thromboprophylaxis for surgical inpatients using variable risk assessment models or other strategies.J Thromb Haemost. 2023 Jun;21(6):1580-1591. doi: 10.1016/j.jtha.2023.02.018. Epub 2023 Mar 1. J Thromb Haemost. 2023. PMID: 36863566
-
Cost effectiveness of enoxaparin as prophylaxis against venous thromboembolic complications in acutely ill medical inpatients: modelling study from the hospital perspective in Germany.Pharmacoeconomics. 2006;24(6):571-91. doi: 10.2165/00019053-200624060-00005. Pharmacoeconomics. 2006. PMID: 16761905
-
A Prospective Observational Cohort of Clinical Outcomes in Medical Inpatients prescribed Pharmacological Thromboprophylaxis Using Different Clinical Risk Assessment Models(COMPT RAMs).Sci Rep. 2019 Dec 4;9(1):18366. doi: 10.1038/s41598-019-54842-3. Sci Rep. 2019. PMID: 31797897 Free PMC article.
-
Multi-gene Pharmacogenomic Testing That Includes Decision-Support Tools to Guide Medication Selection for Major Depression: A Health Technology Assessment.Ont Health Technol Assess Ser. 2021 Aug 12;21(13):1-214. eCollection 2021. Ont Health Technol Assess Ser. 2021. PMID: 34484487 Free PMC article.
-
Retrospective database analysis of the prevention of venous thromboembolism with low-molecular-weight heparin in acutely III medical inpatients in community practice.Clin Ther. 2004 Mar;26(3):419-30. doi: 10.1016/s0149-2918(04)90038-0. Clin Ther. 2004. PMID: 15110135 Review.
Cited by
-
Padua Prediction Score and Hospital-Acquired Proximal and Isolated Distal Deep Vein Thrombosis in Symptomatic Patients.Hematol Rep. 2024 Sep 25;16(4):568-578. doi: 10.3390/hematolrep16040055. Hematol Rep. 2024. PMID: 39449298 Free PMC article.
-
Reply to "Reevaluating thromboprophylaxis in COVID-19 outpatients: the case for a targeted, risk-based approach".Res Pract Thromb Haemost. 2025 Apr 17;9(3):102861. doi: 10.1016/j.rpth.2025.102861. eCollection 2025 Mar. Res Pract Thromb Haemost. 2025. PMID: 40486210 Free PMC article. No abstract available.
References
LinkOut - more resources
Full Text Sources