

Fertility preservation in adult male patients with cancer: a systematic review and meta-analysis
- PMID: 38389980
- PMCID: PMC10882264
- DOI: 10.1093/hropen/hoae006
Fertility preservation in adult male patients with cancer: a systematic review and meta-analysis
Abstract
Study question: Does sperm cryopreservation serve as a feasible and effective method for preserving fertility in adult male patients with cancer?
Summary answer: Sperm cryopreservation is an effective fertility preservation method and may benefit patients with cancer.
What is known already: Sperm cryopreservation is the only way to efficiently preserve male fertility. It is an important procedure in ART. Recently, due to remarkable advances in cancer treatment, an increasing number of studies have reported the outcomes of sperm cryopreservation in patients with cancer.
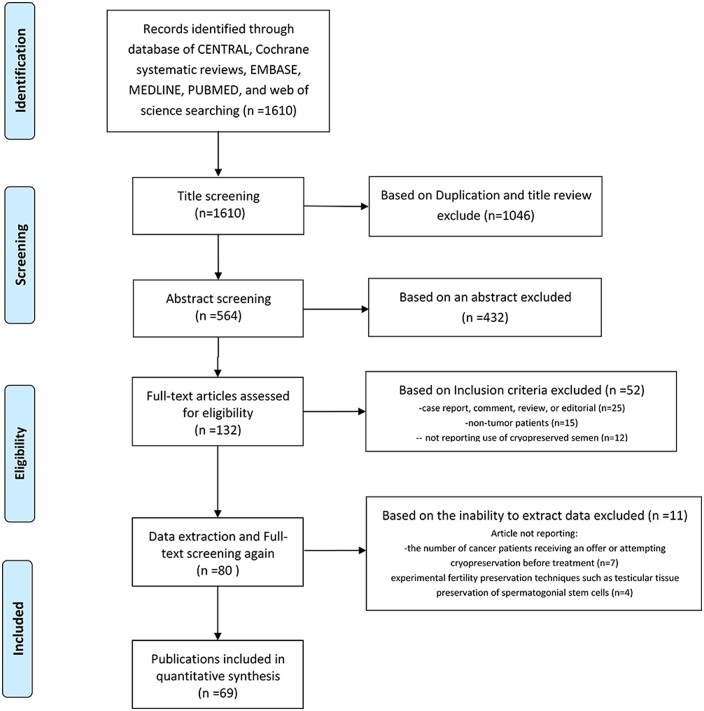
Study design size duration: We conducted an extensive literature search for relevant studies published through to 31 December 2021, in the following databases: CENTRAL, CNKI, Cochrane Systematic Reviews, EMBASE, MEDLINE, PUBMED, and Web of Science. The search terms used were '(cryopreservation OR freeze OR freezing OR banking OR cryostorage OR storage) AND (sperm OR semen OR spermatozoon) AND (cancer OR tumor OR malignancy OR neoplasm)'.
Participants/materials setting methods: We included all studies that reported offering or attempting to cryopreserve sperm before or during cancer treatment in male patients considered at risk of treatment-related fertility impairment. We evaluated the eligibility of all data in each study. The major exclusion criteria were as follows: non-cancer patients; pediatric and adolescent cancer patients; not reporting the use of cryopreserved sperm; use of fresh semen for ART; not reporting the number of patients with cancer offered sperm cryopreservation or attempting to do so before or during treatment; using an experimental fertility preservation technique such as preservation of testicular tissue or spermatogonial stem cells; duplicate data; abstracts, case report, comments, reviews, or editorials; insufficient data reported. The quality of the included studies was assessed using the Newcastle-Ottawa scale and the Methodological Index for Non-Randomized Studies.
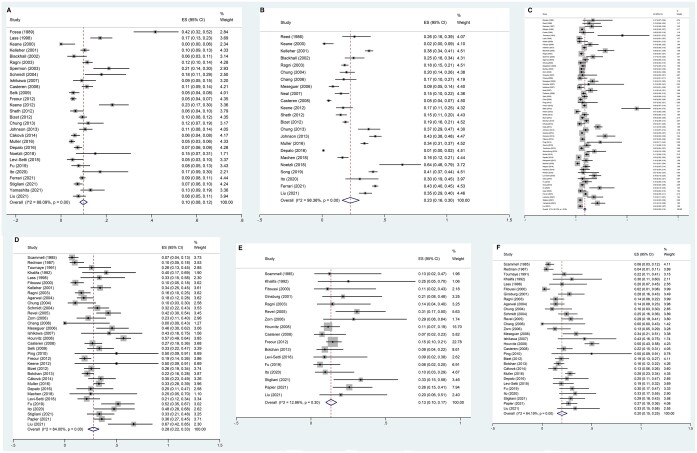
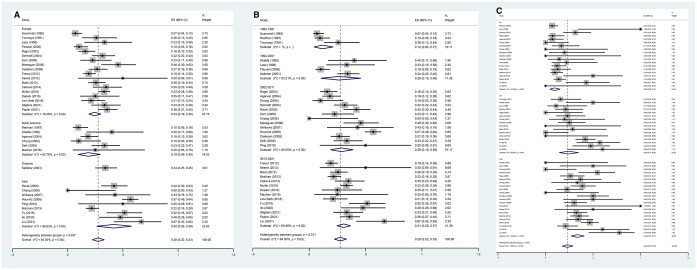
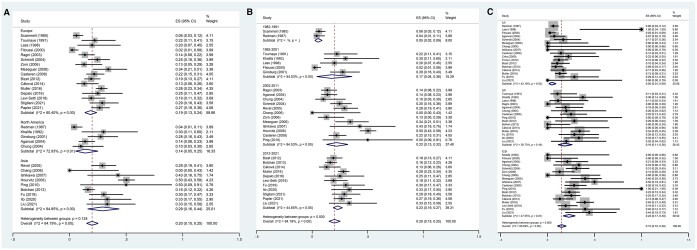
Main results and the role of chance: This meta-analysis included 69 non-randomized studies, with 32 234 patients referred for sperm analysis and 23 178 patients cryopreserving at least one sperm sample. The pooled failed-to-cryopreserve rate was 10% (95% CI, 8-12%), and the sperm disposal and sperm use rates were 23% (95% CI, 16-30%) and 9% (95% CI, 8-10%), respectively. The pregnancy, miscarriage, and delivery rates were 28% (95% CI, 22-33%), 13% (95% CI, 10-17%), and 20% (95% CI, 15-25%), respectively. Subgroup analysis showed higher pregnancy and delivery rates, as well as a lower failed-to-cryopreserve rate, in recent studies compared to those released a decade ago. The studies from Asia reported higher sperm disposal and pregnancy rates than in other continents. Our analysis showed clinical pregnancy rates per cycle of 34% (27-41%), 24% (14-35%), and 9% (5-15%) and delivery rates per cycle of 23% (17-30%), 18% (11-26%), and 5% (1-9%) for ICSI, IVF, and IUI, respectively.
Limitations reasons for caution: As with all meta-analyses, some limitations should be considered. The first limitation of our study is that the data span 36 years. During this time, the World Health Organization has revised its sperm analysis standards, and other important changes have been made. There is also a limitation in that the outcome does not analyze the correlation between the type of cancer and sperm quality. Many of the earlier studies were limited by small sample sizes and a lack of control groups. Furthermore, almost all studies did not consider the severity of the disease, which could potentially have a substantial impact on the results. Consequently, further research should evaluate the effect of the type of cancer and, in particular, the severity of the condition on sperm quality in order to draw more precise conclusions. Similarly, it is inappropriate that most studies failed to differentiate between patients with different types of tumors and instead drew generalized conclusions that are presumed to apply to all patients with cancer. In the present analysis, we did not have in-depth information on patients' disease, and although extensive efforts were made to conduct a thorough systematic review and meta-analysis of the outcomes for patients with various types of tumors, the results must be acknowledged as being subject to bias. However, the use of average results obtained in each study, without the patient-level data, might also represent a source of bias.
Wider implications of the findings: Sperm cryopreservation is an effective fertility preservation method and may benefit patients with cancer. The observed utilization rate of frozen sperm at 9% may underestimate the actual usage, as the short follow-up period is inadequate for obtaining comprehensive data on the use of frozen sperm in young cancer survivors. ART plays an important role in fertility preservation and the achievement of pregnancy, with this meta-analysis showing that ICSI delivers better clinical outcomes than IVF or IUI in patients with cancer undergoing fertility preservation.
Study funding/competing interests: This work was supported by the National Natural Science Foundation of China (grant no. 82001634, 81960550), and the China Postdoctoral Science Foundation (2019M661521). There are no competing interests to declare.
Registration number: CRID 42022314460.
Keywords: cancer; delivery rate; male fertility preservation; meta-analysis; miscarriage rate; pregnancy rate; reproductive outcome; sperm cryopreservation; sperm use rate.
© The Author(s) 2024. Published by Oxford University Press on behalf of European Society of Human Reproduction and Embryology.
Conflict of interest statement
This work was supported by the National Natural Science Foundation of China (grant no. 82001634, 81960550), and the China Postdoctoral Science Foundation (2019M661521). There are no competing interests to declare.The authors have no conflicts of interest to declare.
Figures

Similar articles
-
Safety of fertility preservation techniques before and after anticancer treatments in young women with breast cancer: a systematic review and meta-analysis.Hum Reprod. 2022 May 3;37(5):954-968. doi: 10.1093/humrep/deac035. Hum Reprod. 2022. PMID: 35220429 Free PMC article.
-
A 20-year overview of fertility preservation in boys: new insights gained through a comprehensive international survey.Hum Reprod Open. 2024 Feb 16;2024(2):hoae010. doi: 10.1093/hropen/hoae010. eCollection 2024. Hum Reprod Open. 2024. PMID: 38449521 Free PMC article.
-
Live birth rate after female fertility preservation for cancer or haematopoietic stem cell transplantation: a systematic review and meta-analysis of the three main techniques; embryo, oocyte and ovarian tissue cryopreservation.Hum Reprod. 2023 Mar 1;38(3):489-502. doi: 10.1093/humrep/deac249. Hum Reprod. 2023. PMID: 36421038 Free PMC article.
-
In vitro fertilization and multiple pregnancies: an evidence-based analysis.Ont Health Technol Assess Ser. 2006;6(18):1-63. Epub 2006 Oct 1. Ont Health Technol Assess Ser. 2006. PMID: 23074488 Free PMC article.
-
Sperm cryopreservation does not affect live birth rate in normozoospermic men: analysis of 7969 oocyte donation cycles.Hum Reprod. 2023 Mar 1;38(3):400-407. doi: 10.1093/humrep/dead005. Hum Reprod. 2023. PMID: 36661036
Cited by
-
Does a specific age group impact sperm cryobanking efficiency among adolescent and young adult cancer patients?Obstet Gynecol Sci. 2025 Jul;68(4):323-333. doi: 10.5468/ogs.25009. Epub 2025 Jun 11. Obstet Gynecol Sci. 2025. PMID: 40499583 Free PMC article.
-
The storage time of cryopreserved human spermatozoa does not affect pathways involved in fertility.Basic Clin Androl. 2024 Sep 17;34(1):15. doi: 10.1186/s12610-024-00231-4. Basic Clin Androl. 2024. PMID: 39285325 Free PMC article.
-
[Reproductive Strategies for Declining Fertility: Fertility Preservation].Sichuan Da Xue Xue Bao Yi Xue Ban. 2024 May 20;55(3):507-512. doi: 10.12182/20240560204. Sichuan Da Xue Xue Bao Yi Xue Ban. 2024. PMID: 38948295 Free PMC article. Review. Chinese.
-
An Assessment of Cryopreserved Semen and Testicular Tissue Collected Before and After Cancer Treatment Initiation.Cancer Manag Res. 2024 Jul 24;16:871-882. doi: 10.2147/CMAR.S460960. eCollection 2024. Cancer Manag Res. 2024. PMID: 39077055 Free PMC article.
-
Parenthood in a Swedish prospective cohort of 1,378 adolescents and young adults banking semen for fertility preservation at time of cancer diagnosis.Front Endocrinol (Lausanne). 2024 Dec 10;15:1502479. doi: 10.3389/fendo.2024.1502479. eCollection 2024. Front Endocrinol (Lausanne). 2024. PMID: 39720258 Free PMC article.
References
-
- Agarwal A, Ranganathan P, Kattal N, Pasqualotto F, Hallak J, Khayal S, Mascha E.. Fertility after cancer: a prospective review of assisted reproductive outcome with banked semen specimens. Fertil Steril 2004;81:342–348. - PubMed
-
- Appiah LC. Fertility preservation for adolescents receiving cancer therapies. Clin Obstet Gynecol 2020;63:574–587. - PubMed
-
- Babb A, Farah N, Lyons C, Lindsay K, Reddy N, Goldman J, Apperley JF, Salooja N.. Uptake and outcome of assisted reproductive techniques in long-term survivors of SCT. Bone Marrow Transplant 2012;47:568–573. - PubMed
-
- Bahadur G, Ozturk O, Muneer A, Wafa R, Ashraf A, Jaman N, Patel S, Oyede AW, Ralph DJ.. Semen quality before and after gonadotoxic treatment. Hum Reprod 2005;20:774–781. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials