

Malingering assessment after severe traumatic brain injury in forensic psychology with a potential embedded symptom validity indicator of Symptom Checklist 90
- PMID: 38390415
- PMCID: PMC10882088
- DOI: 10.3389/fpsyg.2024.1320636
Malingering assessment after severe traumatic brain injury in forensic psychology with a potential embedded symptom validity indicator of Symptom Checklist 90
Abstract
Objective: Malingering of neuropsychological damage is common among traumatic brain injury patients pursuing disability compensation in forensic contexts. There is an urgent need to explore differences in neuropsychological assessment outcomes with different levels of cooperation.
Methods: A total of 420 participants with severe traumatic brain injury were classified into malingering group, partial cooperation group, and complete cooperation group according to the Binomial forced-choice digit memory test. The Wechsler Adult Intelligence Scale, event-related potential component, and Symptom Checklist 90 were applied subsequently to assess the psychological status of participants.
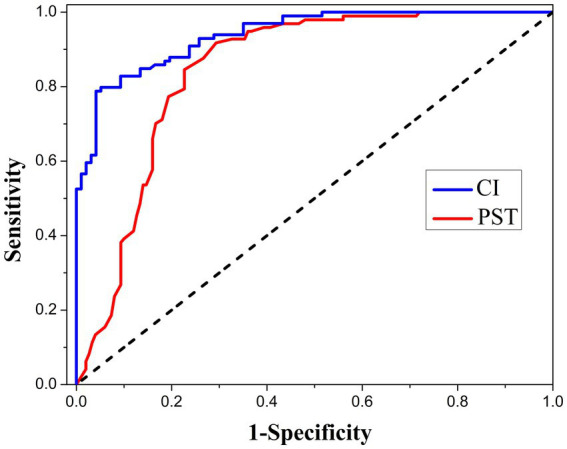
Results: Participants in the malingering group presented lower scores in the binomial forced-choice digit memory test and the Wechsler Adult Intelligence Scale, lower P3 amplitude, and simultaneously higher scores in the Symptom Checklist 90 than the other two groups. The actual intelligence quotient of participants with malingering tendencies ranged mostly between normal and marginal damage, and they often reported elevated whole scale scores in the Symptom Checklist 90. The Cooperation Index (defined as the ratio of positive symptom distress index to global severity index, CI) was proposed and validated to function as an embedded validity indicator of the Symptom Checklist 90, and the area under the receiver operating characteristic (ROC) curve was 0.938. When valued at 1.28, CI has the highest classification ability in differentiating malingering from non-malingering. Combined with the CI and P3 amplitude, the area under the ROC curve for malingering diagnosis further reached 0.952.
Conclusion: Any non-optimal effort in a forensic context will lead to unexpected deviation in psychology evaluation results. CI is a potential candidate to act as an embedded validity indicator of the Symptom Checklist 90. The combination of CI and P3 amplitude can help to identify malingering in participants after severe traumatic brain injury.
Keywords: P300 event-related potentials; Symptoms Checklist 90; disability compensation; forensic psychology; intelligence quotient; malingering; traumatic brain injury.
Copyright © 2024 Liu, Lu, Rao, Chen, Liang and Liu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures




References
-
- Baer R. A., Kroll L. S., Rinaldo J., Ballenger J. (1999). Detecting and discriminating between random responding and overreporting on the MMPI-A. J. Pers. Assess. 72, 308–320. doi: 10.1207/S15327752JP720213 - DOI
-
- Bolzenius J. D., Wade B. S. C., Velez C. S., Drennon A. M., Cooper D. B., Kennedy J. E., et al. . (2018). Relationships between subcortical shape measures and subjective symptom reporting in US service members with mild traumatic brain injury. J. Head Trauma Rehabil. 33, 113–122. doi: 10.1097/HTR.0000000000000379, PMID: - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous