

Duplex Vertical-Flow Rapid Tests for Point-of-Care Detection of Anti-dsDNA and Anti-Nuclear Autoantibodies
- PMID: 38392017
- PMCID: PMC10887294
- DOI: 10.3390/bios14020098
Duplex Vertical-Flow Rapid Tests for Point-of-Care Detection of Anti-dsDNA and Anti-Nuclear Autoantibodies
Abstract
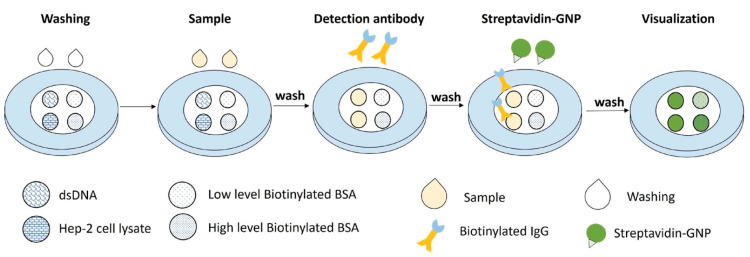
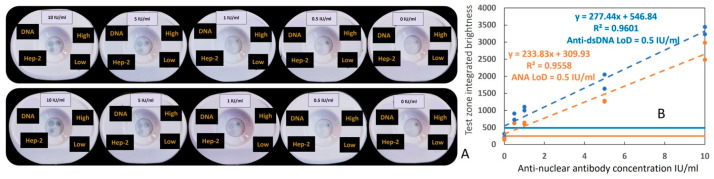
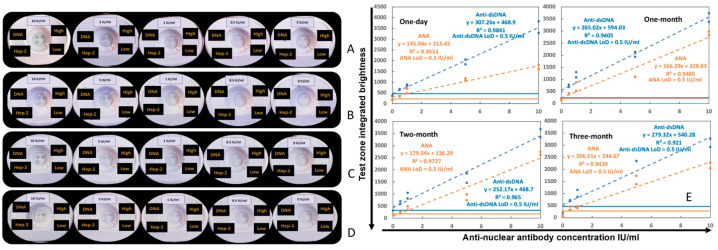
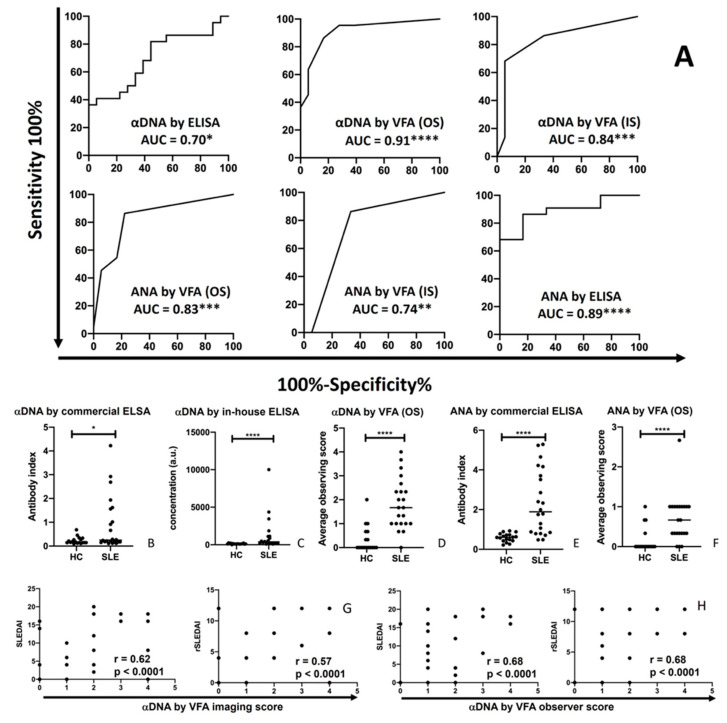
The goal of this study is to develop a rapid diagnostic test for rheumatic disease and systemic lupus erythematosus (SLE) screening. A novel rapid vertical flow assay (VFA) was engineered and used to assay anti-nuclear (ANA) and anti-dsDNA (αDNA) autoantibodies from systemic lupus erythematosus (SLE) patients and healthy controls (HCs). Observer scores and absolute signal intensities from the VFA were validated via ELISA. The rapid point-of-care VFA test that was engineered demonstrated a limit of detection of 0.5 IU/mL for ANA and αDNA autoantibodies in human plasma with an inter-operator CV of 19% for ANA and 12% for αDNA. Storage stability was verified over a three-month period. When testing anti-dsDNA and ANA levels in SLE and HC serum samples, the duplex VFA revealed 95% sensitivity, 72% specificity and an 84% ROC AUC value in discriminating disease groups, comparable to the gold standard, ELISA. The rapid αDNA/ANA duplex VFA can potentially be used in primary care clinics for evaluating patients or at-risk subjects for rheumatic diseases and for planning follow-up testing. Given its low cost, ease, and rapid turnaround, it can also be used to assess SLE prevalence estimates.
Keywords: anti-dsDNA antibody; anti-nuclear antibody; gold nanoparticles; rheumatic disease; vertical-flow assay.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Anti-dsDNA antibodies in systemic lupus erythematosus: A combination of two quantitative methods and the ANA pattern is the most efficient strategy of detection.J Immunol Methods. 2015 Dec;427:30-5. doi: 10.1016/j.jim.2015.09.003. Epub 2015 Sep 25. J Immunol Methods. 2015. PMID: 26407840
-
Sensitivity and specificity of ANA and anti-dsDNA in the diagnosis of systemic lupus erythematosus: a comparison using control sera obtained from healthy individuals and patients with multiple medical problems.Asian Pac J Allergy Immunol. 2013 Dec;31(4):292-8. doi: 10.12932/AP0272.31.4.2013. Asian Pac J Allergy Immunol. 2013. PMID: 24383972
-
Anti-nucleosome antibodies as a disease marker in systemic lupus erythematosus and its correlation with disease activity and other autoantibodies.Indian J Dermatol Venereol Leprol. 2010 Mar-Apr;76(2):145-9. doi: 10.4103/0378-6323.60558. Indian J Dermatol Venereol Leprol. 2010. PMID: 20228543
-
The use of laboratory tests in the diagnosis of SLE.J Clin Pathol. 2000 Jun;53(6):424-32. doi: 10.1136/jcp.53.6.424. J Clin Pathol. 2000. PMID: 10911799 Free PMC article. Review.
-
Antinuclear antibody testing - misunderstood or misbegotten?Nat Rev Rheumatol. 2017 Aug;13(8):495-502. doi: 10.1038/nrrheum.2017.74. Epub 2017 May 25. Nat Rev Rheumatol. 2017. PMID: 28541299 Review.
Cited by
-
Paper-Based Vertical Flow Assays for in Vitro Diagnostics and Environmental Monitoring.ACS Sens. 2025 May 23;10(5):3317-3339. doi: 10.1021/acssensors.5c00668. Epub 2025 May 15. ACS Sens. 2025. PMID: 40372939 Free PMC article. Review.
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
