

Electromagnetic Transmitter-Based Prostate Gating for Dose-Escalated Linac-Based Stereotactic Body Radiation Therapy: An Evaluation of Intrafraction Motion
- PMID: 38392066
- PMCID: PMC10887766
- DOI: 10.3390/curroncol31020072
Electromagnetic Transmitter-Based Prostate Gating for Dose-Escalated Linac-Based Stereotactic Body Radiation Therapy: An Evaluation of Intrafraction Motion
Abstract
Background: Stereotactic Body Radiotherapy (SBRT) is as a standard treatment for prostate cancer (PCa). Tight margins and high dose gradients are needed, and the precise localization of the target is mandatory. Our retrospective study reports our experience regarding the evaluation of intrafraction prostate motion during LINAC-based SBRT evaluated with a novel electromagnetic (EM) tracking device. This device consists of an integrated Foley catheter with a transmitter connected to a receiver placed on the treatment table.
Methods: We analyzed 31 patients who received LINAC-based SBRT using flattening filter-free (FFF) volumetric modulated arc therapy (VMAT). The patients were scheduled to be treated for primary (n = 27) or an intraprostatic recurrent PCa (n = 4). A simulation CT scan was conducted while the patients had a filled bladder (100-150 cc) and an empty rectum, and an EM tracking device was used. The same rectal and bladder conditions were employed during the treatment. The patients received 36.25 Gy delivered over five consecutive fractions on the whole prostate and 40 Gy on the nodule(s) visible via MRI, both delivered with a Simultaneous Integrated Boost approach. The CTV-to-PTV margin was 2 mm for both the identified treatment volumes. Patient positioning was verified with XVI ConeBeam-CT (CBCT) matching before each fraction. When the signals exceeded a 2 mm threshold in any of the three spatial directions, the treatment was manually interrupted. A new XVI CBCT was performed if this offset lasted >20 s.
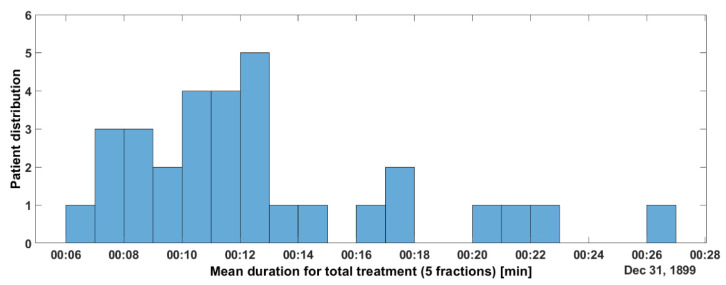
Results: We analyzed data about 155 fractions. The median and mean treatment times, calculated per fraction, were 10 m31 s and 12 m44 s (range: 6 m36 s-65 m28 s), and 95% of the fractions were delivered with a maximum time of 27 m48 s. During treatment delivery, the mean and median number of XVI CBCT operations realized during the treatment were 2 and 1 (range: 0-11). During the treatment, the prostate was outside the CTV-to-PTV margin (2 mm), thus necessitating the stoppage of the delivery +/- a reacquisition of the XVI CBCT for 11.2%, 8.9%, and 3.9% of the delivery time in the vertical, longitudinal, and lateral direction, respectively.
Conclusions: We easily integrated an EM-transmitter-based gating for prostate LINAC-based SBRT into our normal daily workflow. Using this system, a 2 mm CTV-to-PTV margin could be safely applied. A small number of fractions showed a motion exceeding the predefined 2 mm threshold, which would have otherwise gone undetected without intrafraction motion management.
Keywords: extreme hypofractionation; image-guided radiation therapy (IGRT); intrafraction motion mitigation; prostate cancer; real-time electromagnetic tracking; stereotactic body radiation therapy (SBRT).
Conflict of interest statement
The authors declare no conflicts of interest. As declared above, the APC was funded by Micropos Medical AB (Gothenburg, Sweden). The funders had no role in the design, execution, interpretation, or writing of the study.
Figures







References
-
- Miralbell R., Roberts S.A., Zubizarreta E., Hendry J.H. Dose-Fractionation Sensitivity of Prostate Cancer Deduced From Radiotherapy Outcomes of 5969 Patients in Seven International Institutional Datasets: A/b = 1.4 (0.9 − 2.2)Gy. Int. J. Radiat. Oncol. Biol. Phys. 2012;82:e17–e24. doi: 10.1016/j.ijrobp.2010.10.075. - DOI - PubMed
-
- Proust-Lima C., Taylor J.M., Sécher S., Sandler H., Kestin L., Pickles T., Bae K., Allison R., Williams S. Confirmation of a Low a/b Ratio for Prostate Cancer Treated by External Beam Radiation Therapy Alone Using a Post-Treatment Repeated-Measures Model for PSA Dynamics. Int. J. Radiat. Oncol. Biol. Phys. 2011;79:195–201. doi: 10.1016/j.ijrobp.2009.10.008. - DOI - PMC - PubMed
-
- De Bari B., Arcangeli S., Ciardo D., Mazzola R., Alongi F., Russi E.G., Santoni R., Magrini S.M., Jereczek-Fossa B.A., on the behalf of the Italian Association of Radiation Oncology (AIRO) Extreme hypofractionation for early prostate cancer: Biology meets technology. Cancer Treat. Rev. 2016;50:48–60. doi: 10.1016/j.ctrv.2016.08.005. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
