

A Descriptive Analysis of Hybrid Cannulated Extracorporeal Life Support
- PMID: 38392612
- PMCID: PMC10889992
- DOI: 10.3390/jpm14020179
A Descriptive Analysis of Hybrid Cannulated Extracorporeal Life Support
Abstract
Background: Extracorporeal life support (ECLS) is pivotal for sustaining the function of failing hearts and lungs, and its utilization has risen. In cases where conventional cannulation strategies prove ineffective for providing adequate ECLS support, the implementation of an enhanced system with a third cannula may become necessary. Hybrid ECLS may be warranted in situations characterized by severe hypoxemia of the upper extremity, left ventricular congestion, and dilatation. Additionally, it may also be considered for patients requiring respiratory support or experiencing hemodynamic instability.
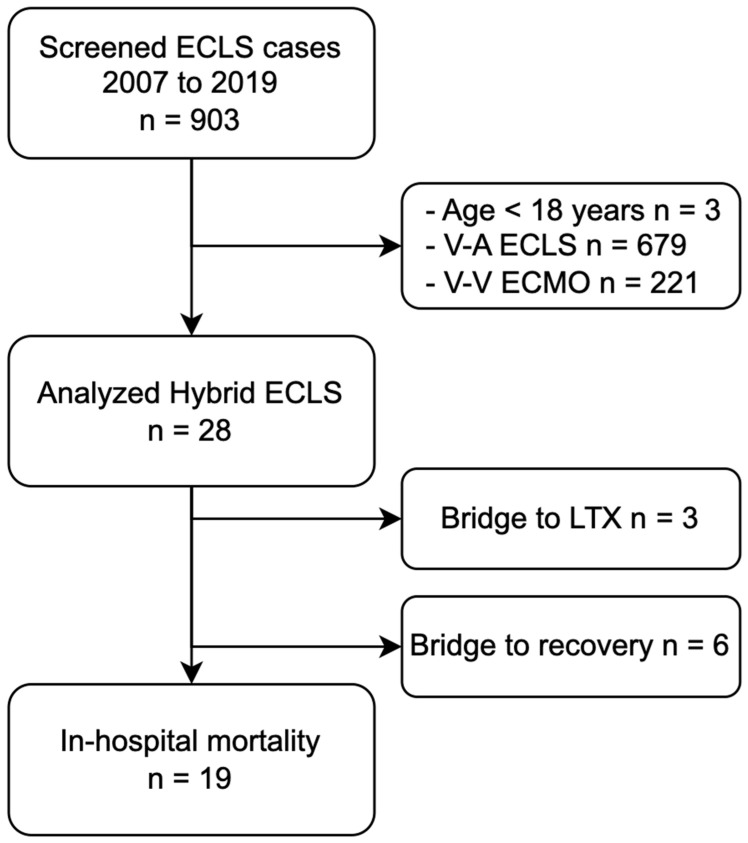
Method: All hybrid ECLS cases of adults at the University Hospital Zurich, Switzerland, between January 2007 and December 2019 with initial triple cannulation were included. Data were collected via a retrospective review of patient records and direct export of the clinical information system.
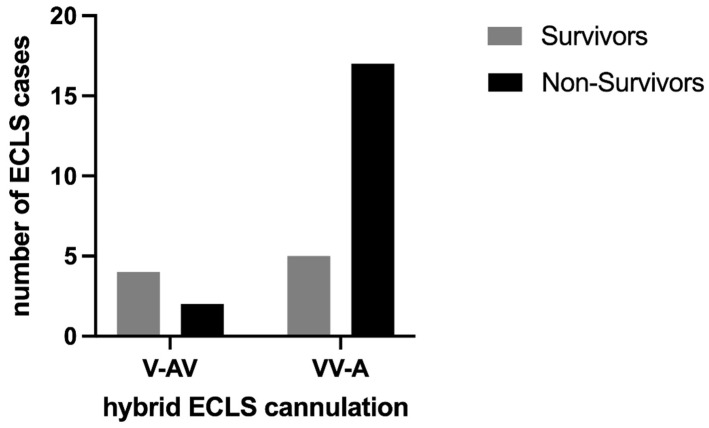
Results: 28 out of 903 ECLS cases were initially hybrid cannulated (3.1%). The median age was 57 (48.2 to 60.8) years, and the sex was equally distributed. The in-hospital mortality of hybrid ECLS was high (67.9%). In-hospital mortality rates differ depending on the indication (ARDS: 36.4%, refractory cardiogenic shock: 88.9%, cardiopulmonary resuscitation: 100%, post-cardiotomy: 100%, others: 75%). Survivors exhibited a lower SAPS II level compared with non-survivors (20.0 (12.0 to 65.0) vs. 55.0 (45.0 to 73.0)), and the allogenic transfusion of platelet concentrate was observed to be less frequent for survivors (0.0 (0.0) vs. 1.8 (2.5) units).
Conclusion: The in-hospital mortality rate for hybrid ECLS was high. Different indications showed varying mortality rates, with survivors having lower SAPS II scores and requiring fewer platelet concentrate transfusions. These findings highlight the complexities of hybrid ECLS outcomes in different clinical scenarios and underline the importance of rigorous patient selection.
Keywords: ECLS; ECMO; extracorporeal circulation; mortality; outcome.
Conflict of interest statement
S.D.S., J.B., R.A. and M.J.W. have no conflicts of interest to declare. A.K. has received support from Bayer AG (Switzerland) and CSL Behring GmbH (Switzerland) for lecturing. D.R.S.’s former academic department receives grant support from the Swiss National Science Foundation, Berne, Switzerland, the Swiss Society of Anesthesiology and Perioperative Medicine (SSAPM), Berne, Switzerland; the Swiss Foundation for Anesthesia Research, Zurich, Switzerland; and CSL Vifor (International) AG, St. Gallen, Switzerland. D.R.S. is co-chair of the ABC-Trauma Faculty, sponsored by unrestricted educational grants from Alexion Pharma Germany GmbH, Munich, Germany; CSL Behring GmbH, Marburg, Germany; and LFB Biomédicaments, Courtaboeuf Cedex, France. D.R.S. received honoraria/travel support for consulting or lecturing from Alliance Rouge, Bern, Switzerland; Danube University of Krems, Austria; European Society of Anesthesiology and Intensive Care, Brussels, BE; International Foundation for Patient Blood Management, Basel, Switzerland; Korean Society of Anesthesiologists, Seoul, Korea; Network for the Advancement of Patient Blood Management, Haemostasis and Thrombosis, Paris, France; Society for the Advancement of Blood Management, Mount Royal NJ, Alexion Pharmaceuticals Inc., Boston, MA; AstraZeneca AG, Baar, Switzerland; Bayer AG, Zürich, Switzerland; B. Braun Melsungen AG, Melsungen, Germany; Baxter AG, Glattpark, Switzerland; CSL Behring GmbH, Hattersheim am Main, Germany and Berne, Switzerland; CSL Vifor (Switzerland) Villars-sur-Glâne, Switzerland; CSL Vifor (International), St. Gallen, Switzerland; Celgene International II Sàrl, Couvet, Switzerland; Daiichi Sankyo AG, Thalwil, Switzerland; Haemonetics, Braintree, MA, USA; iSEP, Nantes, France, LFB Biomédicaments, Courtaboeuf Cedex, France; Merck Sharp & Dohme, Kenilworth, New Jersey, USA; Novo Nordisk Health Care AG, Zurich, Switzerland; Octapharma AG, Lachen, Switzerland; Pharmacosmos A/S, Holbaek, Denmark; Pierre Fabre Pharma, Alschwil, Switzerland; Portola Schweiz GmbH, Aarau, Switzerland; Roche Diagnostics International Ltd., Reinach, Switzerland; Sarstedt AG & Co., Sevelen, Switzerland, and Nümbrecht, Germany; Shire Switzerland GmbH, Zug, Switzerland; Takeda, Glattpark, Switzerland; Werfen, Bedford, MA; and Zuellig Pharma Holdings, Singapore, Singapore.
Figures


References
-
- Assmann A., Beckmann A., Schmid C., Werdan K., Michels G., Miera O., Schmidt F., Klotz S., Starck C., Pilarczyk K., et al. Use of extracorporeal circulation (ECLS/ECMO) for cardiac and circulatory failure -A clinical practice Guideline Level 3. ESC Heart Fail. 2022;9:506–518. doi: 10.1002/ehf2.13718. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
