

Systematic review and meta-analysis of right subclavian artery variants and their correlation with cervical-thoracic clinical conditions
- PMID: 38394517
- PMCID: PMC11309723
- DOI: 10.1097/MD.0000000000036856
Systematic review and meta-analysis of right subclavian artery variants and their correlation with cervical-thoracic clinical conditions
Abstract
Background: A high incidence of anatomical variations in the origin of the branches of the aortic arch has been reported, Nowadays, this variation is considered the most frequent in the aortic arch, its prevalence being estimated between 0.5% and 2.5% of the population. To understand its origin, knowledge of embryonic development is necessary.
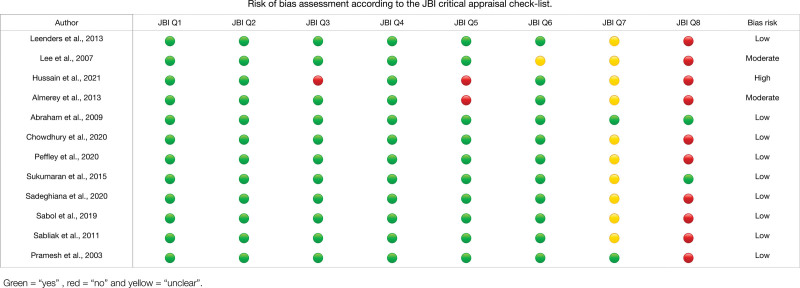
Methods: We searched the MEDLINE, Scopus, Web of Science, Google Scholar, Cumulative Index to Nursing and Allied Health Literature, and Latin-American literature and caribean of health sciences databases with dates ranging from their inception to June 2023. Study selection, data extraction, and methodological quality were assessed with the guaranteed tool for anatomical studies (Anatomical Quality Assurance). Finally, the pooled prevalence was estimated using a random effects model.
Results: Thirty-nine studies were found that met the eligibility criteria. Twenty studies with a total of 41,178 subjects were included in the analysis. The overall prevalence of an ARSA variant was 1% (95% confidence interval = 1%-2%), the clinical findings found are that if ARSA is symptomatic it could produce changes in the hemodynamic function of the thoracocervical region in addition to other associated symptomatic complications in surrounding structures.
Conclusions: ARSA can cause several types of alterations in the cervical or thoracic region, resulting in various clinical complications, such as lusory dysphagia. Hence, knowing this variant is extremely important for surgeons, especially those who treat the cervico-thoracic region. The low prevalence of ARSA means that many professionals are completely unaware of its existence and possible course and origin. Therefore, this study provides detailed knowledge of ARSA so that professionals can make better diagnoses and treatment of ARSA.
Copyright © 2024 the Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures





Similar articles
-
A systematic classification of the left-sided aortic arch variants based on cadaveric studies' prevalence.Surg Radiol Anat. 2021 Mar;43(3):327-345. doi: 10.1007/s00276-020-02625-1. Epub 2021 Jan 2. Surg Radiol Anat. 2021. PMID: 33386933
-
An aberrant right subclavian artery in a 63-year-old male cadaver.Folia Morphol (Warsz). 2023;82(3):726-731. doi: 10.5603/FM.a2022.0085. Epub 2022 Sep 30. Folia Morphol (Warsz). 2023. PMID: 36178279
-
Contemporary management and natural history of aberrant right subclavian artery.J Vasc Surg. 2022 Apr;75(4):1343-1348.e2. doi: 10.1016/j.jvs.2021.11.051. Epub 2021 Nov 24. J Vasc Surg. 2022. PMID: 34838611
-
Association of aberrant subclavian arteries with aortic pathology and proposed classification system.J Vasc Surg. 2020 Nov;72(5):1534-1543. doi: 10.1016/j.jvs.2020.01.042. Epub 2020 Mar 29. J Vasc Surg. 2020. PMID: 32238310
-
A systematic review and meta-analysis: prevalence and clinical implications of anatomical variants of the hepatic portal vein.Sci Rep. 2024 Dec 3;14(1):30002. doi: 10.1038/s41598-024-81543-3. Sci Rep. 2024. PMID: 39622958 Free PMC article.
Cited by
-
Aberrant Right Subclavian Arteries in Dogs Have a Prevalence of 1.2% and Are More Likely to be an Incidental Finding on Computed Tomographic Studies of the Thorax.Vet Radiol Ultrasound. 2025 Mar;66(2):e70011. doi: 10.1111/vru.70011. Vet Radiol Ultrasound. 2025. PMID: 39924899 Free PMC article.
-
CT Angiography for Aortic Arch Anomalies: Prevalence, Diagnostic Efficacy, and Illustrative Findings.Diagnostics (Basel). 2024 Aug 24;14(17):1851. doi: 10.3390/diagnostics14171851. Diagnostics (Basel). 2024. PMID: 39272636 Free PMC article.
-
Conservative Management of Aberrant Right Subclavian Artery (Arteria Lusoria): A Case Report and Literature Review.Cureus. 2025 Apr 19;17(4):e82608. doi: 10.7759/cureus.82608. eCollection 2025 Apr. Cureus. 2025. PMID: 40395245 Free PMC article.
References
-
- Hunauld PM. Examen de quelques parties d’un singe. Hist Acad Roy Sci. 1735;2:516.
-
- Molz G, Burri B. Aberrant subclavian artery (arteria lusoria): sex differences in the prevalence of various forms of the malformation. Evaluation of 1378 observations. Virchows Arch A Pathol Anat Histol. 1978;380:303–15. - PubMed
-
- Zapata H, Edwards JE, Titus JL. Aberrant right subclavian artery with left aortic arch: associated cardiac anomalies. Pediatr Cardiol. 1993;14:159–61. - PubMed
-
- Hegazy A. Clinical Embryology for Medical Students and Postgraduate Doctors. Lap Lambert Academic Publishing; 2014.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
