

Isolated Sagittal Craniosynostosis: A Comprehensive Review
- PMID: 38396475
- PMCID: PMC10887665
- DOI: 10.3390/diagnostics14040435
Isolated Sagittal Craniosynostosis: A Comprehensive Review
Abstract
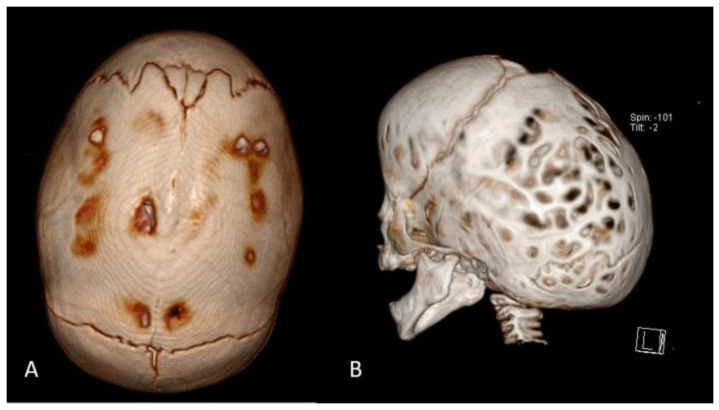
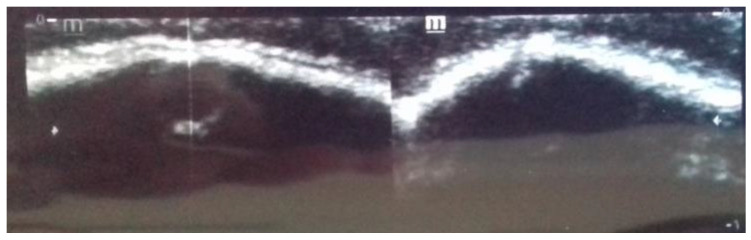
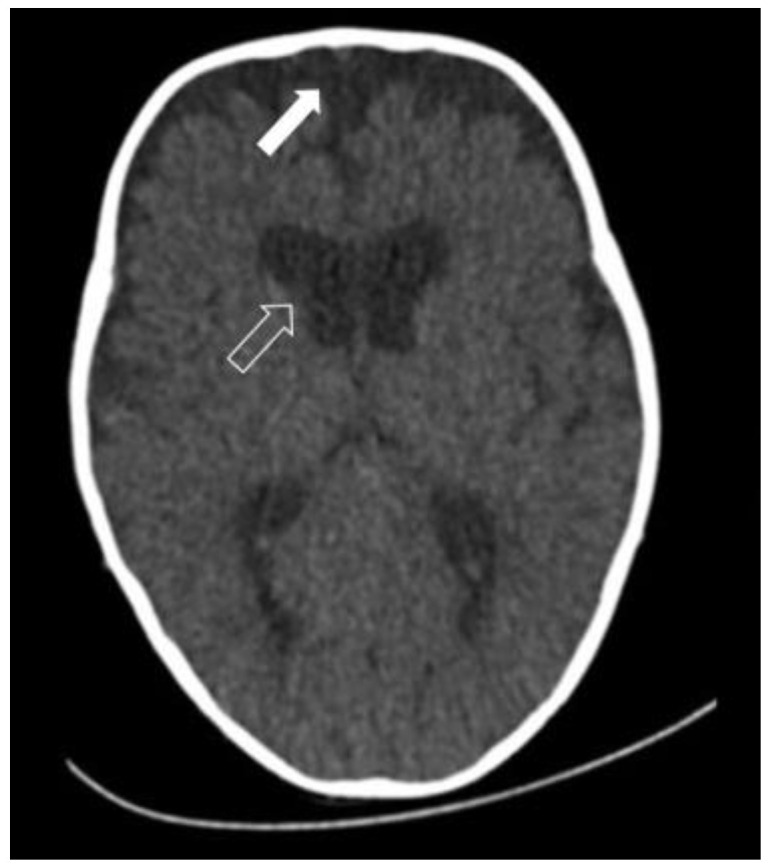
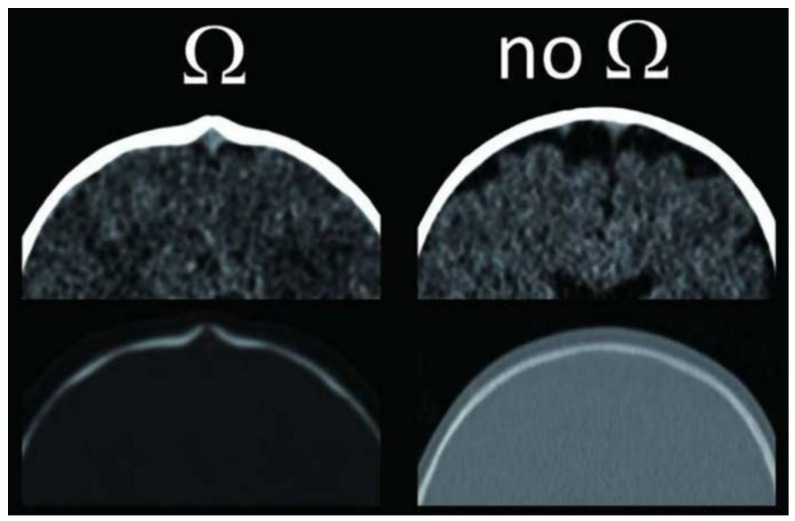
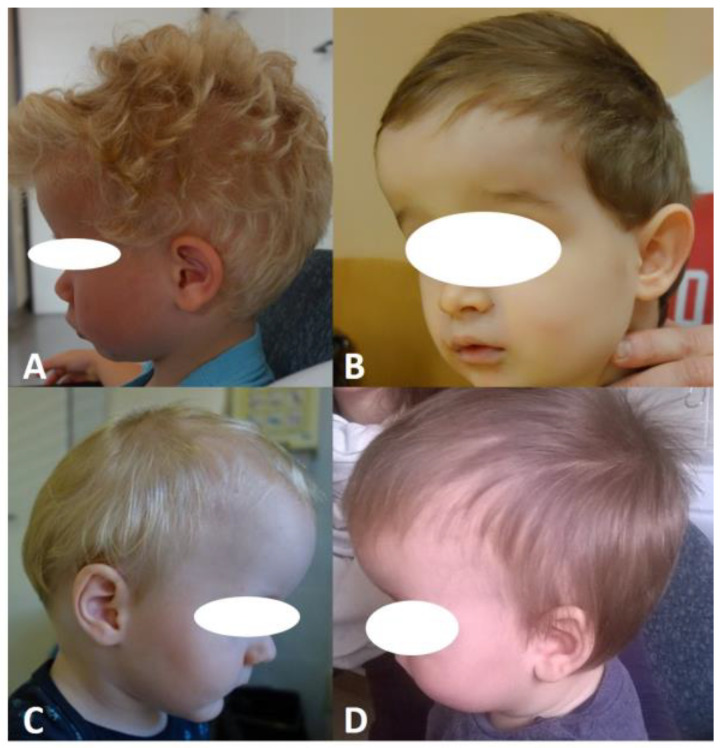
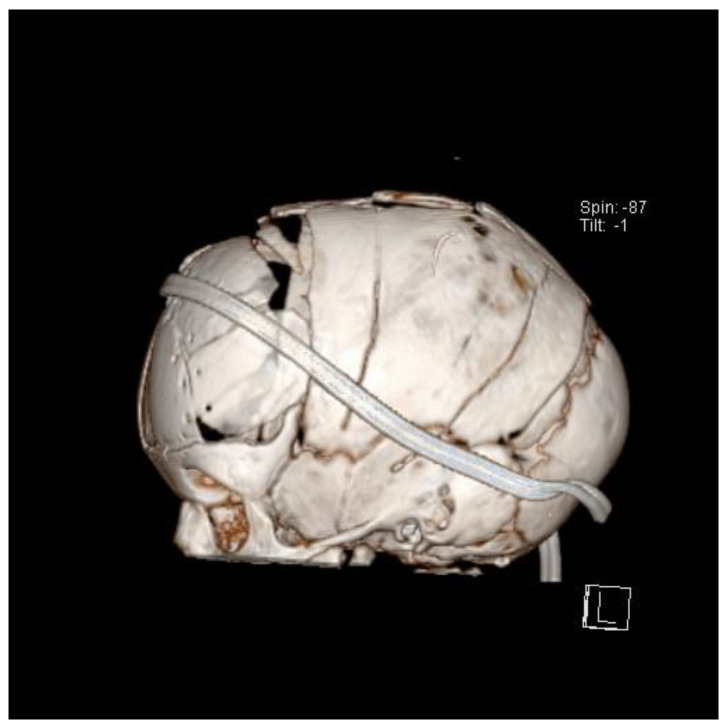
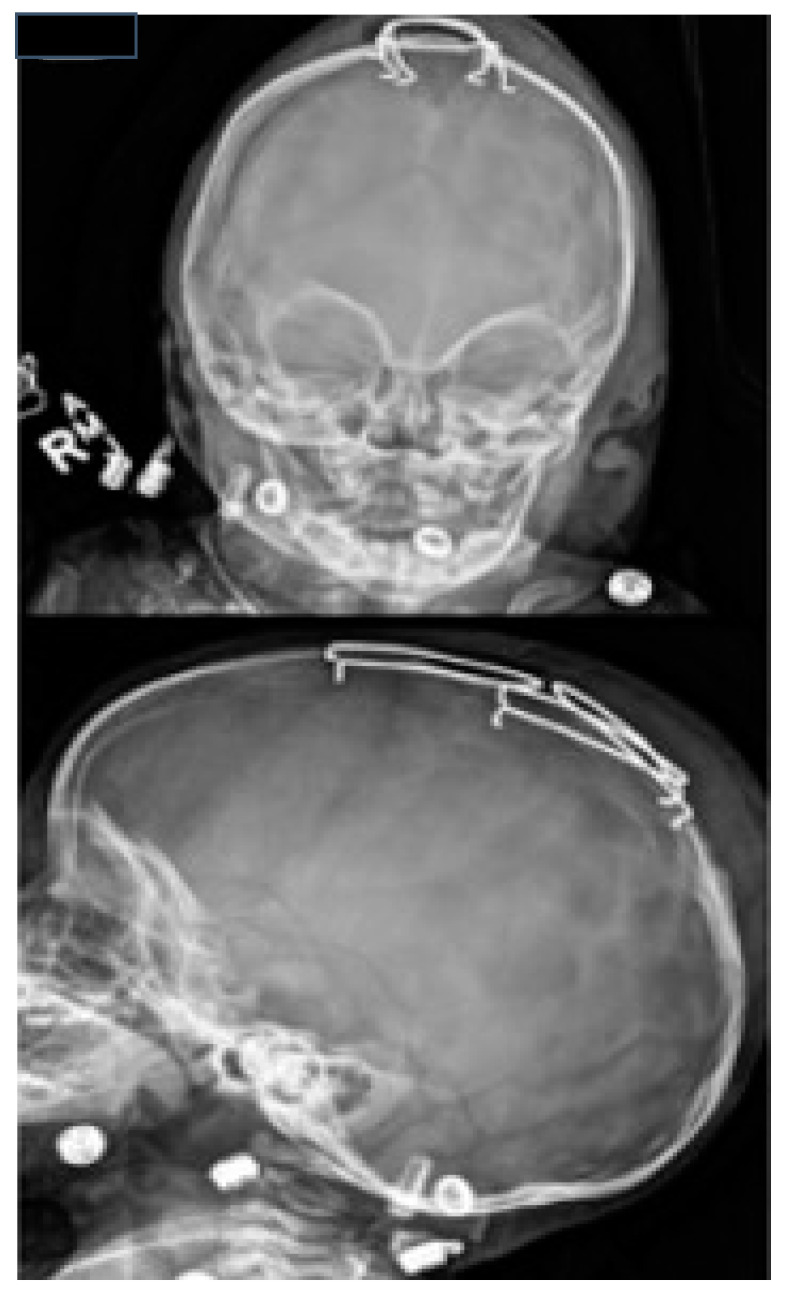
Sagittal craniosynostosis, a rare but fascinating craniofacial anomaly, presents a unique challenge for both diagnosis and treatment. This condition involves premature fusion of the sagittal suture, which alters the normal growth pattern of the skull and can affect neurological development. Sagittal craniosynostosis is characterised by a pronounced head shape, often referred to as scaphocephaly. Asymmetry of the face and head, protrusion of the fontanel, and increased intracranial pressure are common clinical manifestations. Early recognition of these features is crucial for early intervention, and understanding the aetiology is, therefore, essential. Although the exact cause remains unclear, genetic factors are thought to play an important role. Mutations in genes such as FGFR2 and FGFR3, which disrupt the normal development of the skull, are suspected. Environmental factors and various insults during pregnancy can also contribute to the occurrence of the disease. An accurate diagnosis is crucial for treatment. Imaging studies such as ultrasound, computed tomography, magnetic resonance imaging, and three-dimensional reconstructions play a crucial role in visualising the prematurely fused sagittal suture. Clinicians also rely on a physical examination and medical history to confirm the diagnosis. Early detection allows for quick intervention and better treatment outcomes. The treatment of sagittal craniosynostosis requires a multidisciplinary approach that includes neurosurgery, craniofacial surgery, and paediatric care. Traditional treatment consists of an open reconstruction of the cranial vault, where the fused suture is surgically released to allow normal growth of the skull. However, advances in minimally invasive techniques, such as endoscopic strip craniectomy, are becoming increasingly popular due to their lower morbidity and shorter recovery times. This review aims to provide a comprehensive overview of sagittal craniosynostosis, highlighting the aetiology, clinical presentation, diagnostic methods, and current treatment options.
Keywords: cranial deformation; cranial vault remodelling; craniosynostosis; scaphocephaly; surgery.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures


Similar articles
-
Management of Sagittal and Lambdoid Craniosynostosis: Open Cranial Vault Expansion and Remodeling.Oral Maxillofac Surg Clin North Am. 2022 Aug;34(3):395-419. doi: 10.1016/j.coms.2022.01.005. Epub 2022 Jun 23. Oral Maxillofac Surg Clin North Am. 2022. PMID: 35752548 Review.
-
Posterior Cranial Vault Manifestations in Nonsyndromic Sagittal Craniosynostosis.J Craniofac Surg. 2021 Oct 1;32(7):2273-2276. doi: 10.1097/SCS.0000000000007756. J Craniofac Surg. 2021. PMID: 34054080
-
Postnatal Sagittal Craniosynostosis: A Novel Presentation and Considerations in Diagnosis and Management.J Craniofac Surg. 2021 Oct 1;32(7):2452-2455. doi: 10.1097/SCS.0000000000007599. J Craniofac Surg. 2021. PMID: 33654043
-
Craniosynostosis - A Review for Providers.S D Med. 2021 Feb;74(2):83-88. S D Med. 2021. PMID: 34161690
-
MOC-PS(SM) CME article: management considerations in the treatment of craniosynostosis.Plast Reconstr Surg. 2008 Apr;121(4 Suppl):1-11. doi: 10.1097/01.prs.0000305929.40363.bf. Plast Reconstr Surg. 2008. PMID: 18379381 Review.
Cited by
-
Developments in diagnostic and surgical techniques in children with sagittal suture craniosynostosis: a systematic review spanning the last 30 years.Orphanet J Rare Dis. 2025 Aug 17;20(1):437. doi: 10.1186/s13023-025-03978-9. Orphanet J Rare Dis. 2025. PMID: 40820202 Free PMC article. Review.
-
Concurrent myelomeningocele and sagittal craniosynostosis: illustrative case.J Neurosurg Case Lessons. 2025 Jan 6;9(1):CASE24616. doi: 10.3171/CASE24616. Print 2025 Jan 6. J Neurosurg Case Lessons. 2025. PMID: 39761544 Free PMC article.
-
Endoscopic versus open treatment for sagittal craniosynostosis: a systematic review and meta-analysis.Neurosurg Rev. 2025 Feb 22;48(1):262. doi: 10.1007/s10143-025-03423-2. Neurosurg Rev. 2025. PMID: 39984767
References
-
- Spazzapan P., Kočar M., Eberlinc A., Velnar T. Kraniofacialne rekonstrukcije pri otrocih s kraniosinostozo. Slov. Pediatr. 2021;28:67–77. doi: 10.38031/slovpediatr-2021-2-01. - DOI
-
- Virchow R. Uber den Cretinismus, namentlich in Franken, und uber pathologische Schadelformen. Verh. Phys. Med. Ges. Wurzbg. 1851;2:230.
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
