

Insights into Hyperparathyroidism-Jaw Tumour Syndrome: From Endocrine Acumen to the Spectrum of CDC73 Gene and Parafibromin-Deficient Tumours
- PMID: 38396977
- PMCID: PMC10889221
- DOI: 10.3390/ijms25042301
Insights into Hyperparathyroidism-Jaw Tumour Syndrome: From Endocrine Acumen to the Spectrum of CDC73 Gene and Parafibromin-Deficient Tumours
Abstract
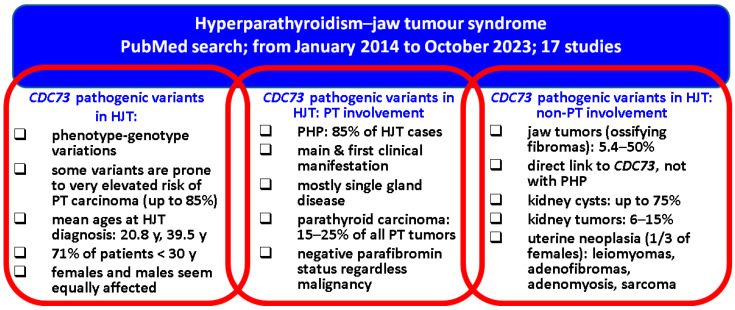
A total of 1 out of 10 patients with primary hyperparathyroidism (PHP) presents an underlying genetic form, such as multiple endocrine neoplasia types 1, 2A, etc., as well as hyperparathyroidism-jaw tumour syndrome (HJT). We aimed to summarise the recent data, thus raising more awareness regarding HJT, from the clinical perspective of PHP in association with the challenges and pitfalls of CDC73 genetic testing and parafibromin staining. This narrative review included a sample-focused analysis from the past decade according to a PubMed search. We identified 17 original human studies (≥4 patients per article). The mean age at disease onset was between 20.8 and 39.5 years, while the largest study found that 71% of patients had HJT recognised before the age of 30. Males and females seemed to be equally affected, in contrast with sporadic PHP. PHP represented the central manifestation of HJT, occurring as the first manifestation in up to 85% of HJT cases. A biochemistry panel found a mean serum calcium level above the level of 12 mg/dL in PHP. PTH was elevated in HJT as well, with average values of at least 236.6 pg/mL. The most frequent pathological type in PHP was a parathyroid adenoma, but the incidence of a parathyroid carcinoma was much higher than in non-HJT cases (15% of all parathyroid tumours), with the diagnosis being established between the age of 15 and 37.5. In some families up to 85% of carriers suffered from a parathyroid carcinoma thus indicating that certain CDC73 pathogenic variants may harbour a higher risk. An important issue in HJT was represented by the parafibromin profile in the parathyroid tumours since in HJT both parathyroid adenomas and carcinomas might display a deficient immunoreactivity. Another frequent manifestation in HJT was ossifying fibromas of the jaw (affecting 5.4% to 50% of patients; the largest study found a prevalence of 15.4%). HJT was associated with a wide variety of kidney lesion (mostly: kidney cysts, with a prevalence of up to 75%, and renal tumours involved in 19% of patients). The risk of uterine lesions seemed increased in HJT, especially with concern to leiomyomas, adenofibromas, and adenomyosis. The underlying pathogenic mechanisms and the involvement of CDC73 pathogenic variants and parafibromin expression are yet to be explored. Currently, the heterogeneous expression of parafibromin status and, the wide spectrum of CDC73 mutations including the variety of clinical presentations in HJT, make it difficult to predict the phenotype based on the genotype. The central role of HJT-PHP is, however, the main clinical element, while the elevated risk of parathyroid carcinoma requires a special awareness.
Keywords: CDC73; gene; hyperparathyroidism–jaw tumour syndrome; immunohistochemistry; jaw tumour; parafibromin; parathyroid carcinoma; parathyroid tumour; parathyroidectomy.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Mice deleted for cell division cycle 73 gene develop parathyroid and uterine tumours: model for the hyperparathyroidism-jaw tumour syndrome.Oncogene. 2017 Jul 13;36(28):4025-4036. doi: 10.1038/onc.2017.43. Epub 2017 Mar 13. Oncogene. 2017. PMID: 28288139 Free PMC article.
-
Characterization of a novel CDC73 gene mutation in a hyperparathyrodism-jaw tumor patient affected by parathyroid carcinoma in the absence of somatic loss of heterozygosity.Endocr J. 2019 Apr 25;66(4):319-327. doi: 10.1507/endocrj.EJ18-0387. Epub 2019 Feb 22. Endocr J. 2019. PMID: 30799315
-
Tumor suppressor gene mutation in a patient with a history of hyperparathyroidism-jaw tumor syndrome and healed generalized osteitis fibrosa cystica: a case report and genetic pathophysiology review.J Oral Maxillofac Surg. 2015 Jan;73(1):194.e1-9. doi: 10.1016/j.joms.2014.09.008. Epub 2014 Sep 28. J Oral Maxillofac Surg. 2015. PMID: 25511968 Review.
-
A novel CDC73 gene mutation in an Italian family with hyperparathyroidism-jaw tumour (HPT-JT) syndrome.Cell Oncol (Dordr). 2014 Aug;37(4):281-8. doi: 10.1007/s13402-014-0187-3. Epub 2014 Aug 12. Cell Oncol (Dordr). 2014. PMID: 25113791
-
Association Between Parafibromin Expression and Presence of Brown Tumors and Jaw Tumors in Patients with Primary Hyperparathyroidism: Series of Cases with Review of the Literature.Am J Case Rep. 2022 Oct 22;23:e936135. doi: 10.12659/AJCR.936135. Am J Case Rep. 2022. PMID: 36271606 Free PMC article. Review.
Cited by
-
Progress report on multiple endocrine neoplasia type 1.Fam Cancer. 2025 Jan 18;24(1):15. doi: 10.1007/s10689-025-00440-4. Fam Cancer. 2025. PMID: 39826015 Free PMC article. Review.
-
Rare genetic disorders that impair parathyroid hormone synthesis, secretion, or bioactivity provide insights into the diagnostic utility of different parathyroid hormone assays.Curr Opin Nephrol Hypertens. 2024 Jul 1;33(4):375-382. doi: 10.1097/MNH.0000000000000999. Epub 2024 May 3. Curr Opin Nephrol Hypertens. 2024. PMID: 38701324 Free PMC article. Review.
-
The Delicate Balancing of Pros and Cons in the Surgical Management of Hyperparathyroidism in a Young Female with Germline Variant in the CDC73 Gene.Calcif Tissue Int. 2025 Jan 3;116(1):21. doi: 10.1007/s00223-024-01334-w. Calcif Tissue Int. 2025. PMID: 39751933 Free PMC article.
References
-
- Medina J.E., Randolph G.W., Angelos P., Zafereo M.E., Tufano R.P., Kowalski L.P., Montenegro F.L.M., Owen R.P., Khafif A., Suárez C., et al. Primary hyperparathyroidism: Disease of diverse genetic, symptomatic, and biochemical phenotypes. Head Neck. 2021;43:3996–4009. doi: 10.1002/hed.26861. - DOI - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
