

Unveiling the Protective Role of Melatonin in Osteosarcoma: Current Knowledge and Limitations
- PMID: 38397382
- PMCID: PMC10886489
- DOI: 10.3390/biom14020145
Unveiling the Protective Role of Melatonin in Osteosarcoma: Current Knowledge and Limitations
Abstract
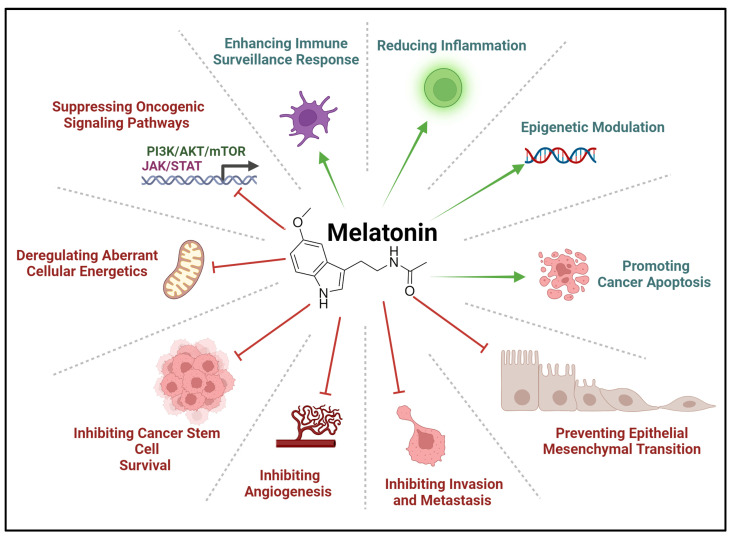
Melatonin, an endogenous neurohormone produced by the pineal gland, has received increased interest due to its potential anti-cancer properties. Apart from its well-known role in the sleep-wake cycle, extensive scientific evidence has shown its role in various physiological and pathological processes, such as inflammation. Additionally, melatonin has demonstrated promising potential as an anti-cancer agent as its function includes inhibition of tumorigenesis, induction of apoptosis, and regulation of anti-tumor immune response. Although a precise pathophysiological mechanism is yet to be established, several pathways related to the regulation of cell cycle progression, DNA repair mechanisms, and antioxidant activity have been implicated in the anti-neoplastic potential of melatonin. In the current manuscript, we focus on the potential anti-cancer properties of melatonin and its use in treating and managing pediatric osteosarcoma. This aggressive bone tumor primarily affects children and adolescents and is treated mainly by surgical and radio-oncological interventions, which has improved survival rates among affected individuals. Significant disadvantages to these interventions include disease recurrence, therapy-related toxicity, and severe/debilitating side effects that the patients have to endure, significantly affecting their quality of life. Melatonin has therapeutic effects when used for treating osteosarcoma, attributed to its ability to halt cancer cell proliferation and trigger apoptotic cell death, thereby enhancing chemotherapeutic efficacy. Furthermore, the antioxidative function of melatonin alleviates harmful side effects of chemotherapy-induced oxidative damage, aiding in decreasing therapeutic toxicities. The review concisely explains the many mechanisms by which melatonin targets osteosarcoma, as evidenced by significant results from several in vitro and animal models. Nevertheless, if further explored, human trials remain a challenge that could shed light and support its utility as an adjunctive therapeutic modality for treating osteosarcoma.
Keywords: anti-cancer therapeutics; apoptosis; bone cancer; melatonin; osteosarcoma.
Conflict of interest statement
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the article.
Figures





References
-
- Arendt J., Aulinas A. Physiology of the Pineal Gland and Melatonin. In: Feingold K.R., Anawalt B., Blackman M.R., Boyce A., Chrousos G., Corpas E., de Herder W.W., Dhatariya K., Dungan K., Hofland J., et al., editors. Endotext. MDText.com, Inc.; South Dartmouth, MA, USA: 2000. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
