

Gender Influence on XOR Activities and Related Pathologies: A Narrative Review
- PMID: 38397809
- PMCID: PMC10885918
- DOI: 10.3390/antiox13020211
Gender Influence on XOR Activities and Related Pathologies: A Narrative Review
Abstract
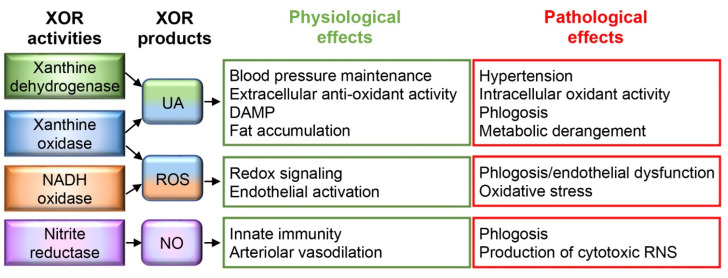
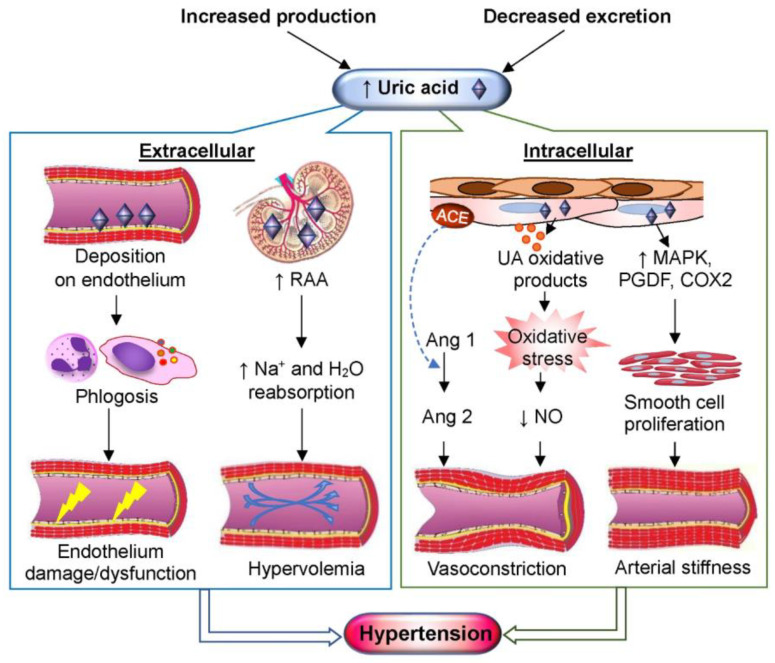
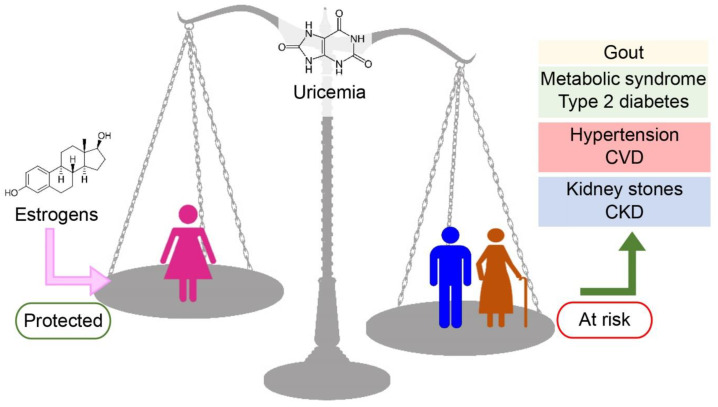
Taking into account the patient's gender is the first step towards more precise and egalitarian medicine. The gender-related divergences observed in purine catabolism and their pathological consequences are good examples of gender medicine differences. Uric acid is produced by the activity of xanthine oxidoreductase (XOR). The serum levels of both XOR activity and uric acid differ physiologically between the genders, being higher in men than in women. Their higher levels have been associated with gout and hypertension, as well as with vascular, cardiac, renal, and metabolic diseases. The present review analyzes the gender-related differences in these pathological conditions in relation to increases in the serum levels of XOR and/or uric acid and the opportunity for gender-driven pharmacological treatment.
Keywords: cardiovascular disease; chronic kidney disease; gender medicine; gout; hypertension; metabolic syndrome; uric acid; xanthine oxidoreductase.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Committee 2 of the International Commission on Radiological Protection . Report on the Task Group on Reference Man. Pergamon Press; New York, NY, USA: 1975.
Publication types
LinkOut - more resources
Full Text Sources
