

Genetic Susceptibility to Arrhythmia Phenotypes in a Middle Eastern Cohort of 14,259 Whole-Genome Sequenced Individuals
- PMID: 38398418
- PMCID: PMC10888535
- DOI: 10.3390/jcm13041102
Genetic Susceptibility to Arrhythmia Phenotypes in a Middle Eastern Cohort of 14,259 Whole-Genome Sequenced Individuals
Abstract
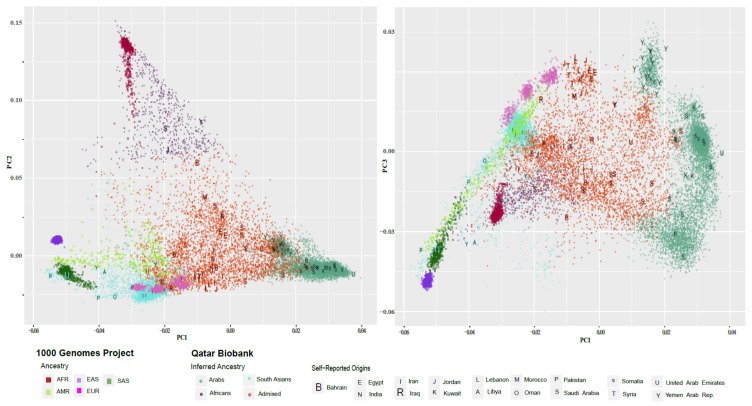
Background: The current study explores the genetic underpinnings of cardiac arrhythmia phenotypes within Middle Eastern populations, which are under-represented in genomic medicine research. Methods: Whole-genome sequencing data from 14,259 individuals from the Qatar Biobank were used and contained 47.8% of Arab ancestry, 18.4% of South Asian ancestry, and 4.6% of African ancestry. The frequency of rare functional variants within a set of 410 candidate genes for cardiac arrhythmias was assessed. Polygenic risk score (PRS) performance for atrial fibrillation (AF) prediction was evaluated. Results: This study identified 1196 rare functional variants, including 162 previously linked to arrhythmia phenotypes, with varying frequencies across Arab, South Asian, and African ancestries. Of these, 137 variants met the pathogenic or likely pathogenic (P/LP) criteria according to ACMG guidelines. Of these, 91 were in ACMG actionable genes and were present in 1030 individuals (~7%). Ten P/LP variants showed significant associations with atrial fibrillation p < 2.4 × 10-10. Five out of ten existing PRSs were significantly associated with AF (e.g., PGS000727, p = 0.03, OR = 1.43 [1.03, 1.97]). Conclusions: Our study is the largest to study the genetic predisposition to arrhythmia phenotypes in the Middle East using whole-genome sequence data. It underscores the importance of including diverse populations in genomic investigations to elucidate the genetic landscape of cardiac arrhythmias and mitigate health disparities in genomic medicine.
Keywords: Middle East; arrythmia; atrial fibrillation; cardiomyopathy; diverse populations; diversity; genomics; whole-genome sequencing.
Conflict of interest statement
Amar Salam, Jassim Al Suwaidi, and Nidal Asaad are employed by Hamad Medical Corporation. All of the authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as potential conflicts of interest.
Figures




Similar articles
-
Genetic predisposition to cancer across people of different ancestries in Qatar: a population-based, cohort study.Lancet Oncol. 2022 Mar;23(3):341-352. doi: 10.1016/S1470-2045(21)00752-X. Epub 2022 Feb 9. Lancet Oncol. 2022. PMID: 35150601
-
Actionable genomic variants in 6045 participants from the Qatar Genome Program.Hum Mutat. 2021 Aug 24. doi: 10.1002/humu.24278. Online ahead of print. Hum Mutat. 2021. PMID: 34428338
-
Polygenic risk scores for the prediction of common cancers in East Asians: A population-based prospective cohort study.Elife. 2023 Mar 27;12:e82608. doi: 10.7554/eLife.82608. Elife. 2023. PMID: 36971353 Free PMC article.
-
[Genetic basis of atrial fibrillation-on the road to precision medicine].Herzschrittmacherther Elektrophysiol. 2024 Mar;35(1):3-8. doi: 10.1007/s00399-023-00974-z. Epub 2023 Nov 6. Herzschrittmacherther Elektrophysiol. 2024. PMID: 37932605 Free PMC article. Review. German.
-
Genetically based atrial fibrillation: Current considerations for diagnosis and management.J Cardiovasc Electrophysiol. 2022 Aug;33(8):1944-1953. doi: 10.1111/jce.15446. Epub 2022 Mar 19. J Cardiovasc Electrophysiol. 2022. PMID: 35262243 Review.
Cited by
-
Genome-Wide Association Study for Resting Electrocardiogram in the Qatari Population Identifies 6 Novel Genes and Validates Novel Polygenic Risk Scores.J Am Heart Assoc. 2025 Mar 4;14(5):e038341. doi: 10.1161/JAHA.124.038341. Epub 2025 Feb 26. J Am Heart Assoc. 2025. PMID: 40008532 Free PMC article.
References
-
- January C.T., Wann L.S., Alpert J.S., Calkins H., Cigarroa J.E., Cleveland J.C., Jr., Conti J.B., Ellinor P.T., Ezekowitz M.D., Field M.E., et al. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. J. Am. Coll. Cardiol. 2014;64:e1–e76. doi: 10.1016/j.jacc.2014.03.022. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
