

Severe Lung Dysfunction and Pulmonary Blood Flow during Extracorporeal Membrane Oxygenation
- PMID: 38398425
- PMCID: PMC10889439
- DOI: 10.3390/jcm13041113
Severe Lung Dysfunction and Pulmonary Blood Flow during Extracorporeal Membrane Oxygenation
Abstract
Background: Extracorporeal membrane oxygenation (ECMO) is indicated for patients with severe respiratory and/or circulatory failure. The standard technique to visualize the extent of pulmonary damage during ECMO is computed tomography (CT).
Purpose: This single-center, retrospective study investigated whether pulmonary blood flow (PBF) measured with echocardiography can assist in assessing the extent of pulmonary damage and whether echocardiography and CT findings are associated with patient outcomes.
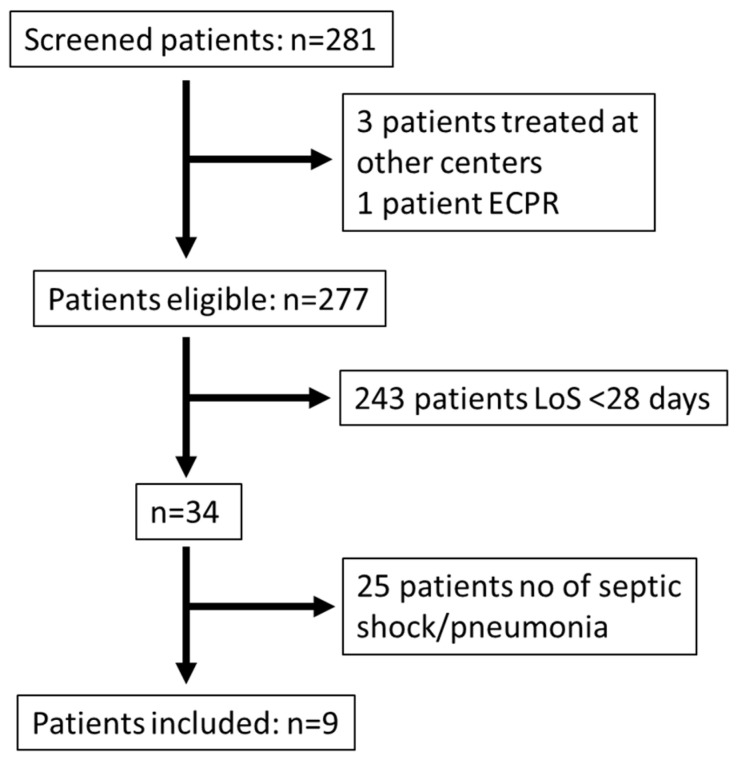
Methods: All patients (>15 years) commenced on ECMO between 2011 and 2017 with septic shock of pulmonary origin and a treatment time >28 days were screened. Of 277 eligible patients, 9 were identified where both CT and echocardiography had been consecutively performed.
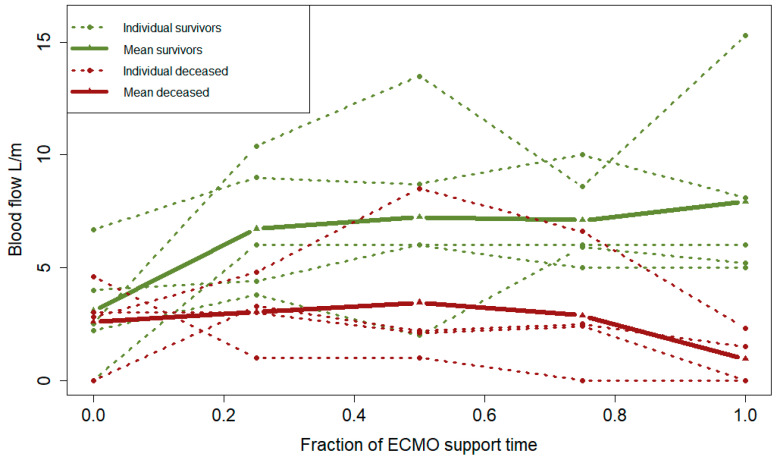
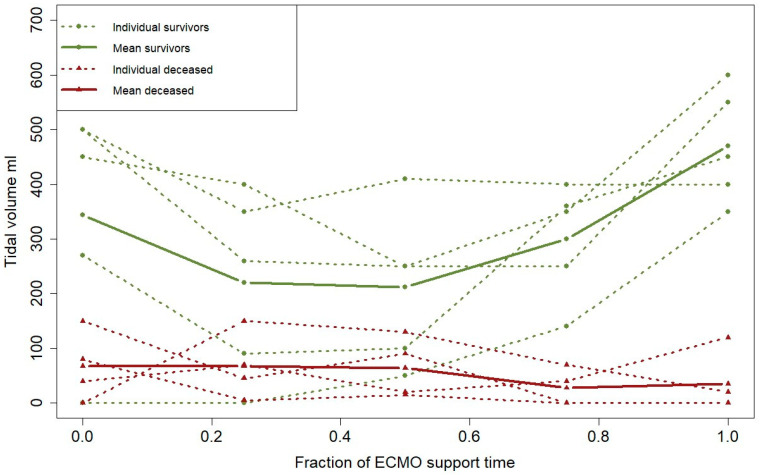
Results: CT failed to indicate any differences in viable lung parenchyma within or between survivors and non-survivors at any time during ECMO treatment. Upon initiation of ECMO, the survivors (n = 5) and non-survivors (n = 4) had similar PBF. During a full course of ECMO support, survivors showed no change in PBF (3.8 ± 2.1 at ECMO start vs. 7.9 ± 4.3 L/min, p = 0.12), whereas non-survivors significantly deteriorated in PBF from 3.5 ± 1.0 to 1.0 ± 1.1 L/min (p = 0.029). Tidal volumes were significantly lower over time among the non-survivors, p = 0.047.
Conclusions: In prolonged ECMO for pulmonary septic shock, CT was not found to be effective for the evaluation of pulmonary viability or recovery. This hypothesis-generating investigation supports echocardiography as a tool to predict pulmonary recovery via the assessment of PBF at the early to later stages of ECMO support.
Keywords: extracorporeal membrane oxygenation; prognosis; prognostication; prolonged ECMO; pulmonary blood flow; sepsis; septic shock; tidal volume.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Extracorporeal lung support technologies - bridge to recovery and bridge to lung transplantation in adult patients: an evidence-based analysis.Ont Health Technol Assess Ser. 2010;10(5):1-47. Epub 2010 Apr 1. Ont Health Technol Assess Ser. 2010. PMID: 23074408 Free PMC article.
-
Venoarterial extracorporeal membrane oxygenation is an effective management strategy for massive pulmonary embolism patients.J Vasc Surg Venous Lymphat Disord. 2021 Mar;9(2):307-314. doi: 10.1016/j.jvsv.2020.04.033. Epub 2020 Jun 4. J Vasc Surg Venous Lymphat Disord. 2021. PMID: 32505687
-
Venoarterial extracorporeal membrane oxygenation to rescue sepsis-induced cardiogenic shock: a retrospective, multicentre, international cohort study.Lancet. 2020 Aug 22;396(10250):545-552. doi: 10.1016/S0140-6736(20)30733-9. Lancet. 2020. PMID: 32828186
-
Extracorporeal Membrane Oxygenation for Septic Shock in Adults and Children: A Narrative Review.J Clin Med. 2023 Oct 20;12(20):6661. doi: 10.3390/jcm12206661. J Clin Med. 2023. PMID: 37892799 Free PMC article. Review.
-
Extracorporeal membrane oxygenation in the treatment of poisoned patients.Clin Toxicol (Phila). 2013 Jun;51(5):385-93. doi: 10.3109/15563650.2013.800876. Epub 2013 May 23. Clin Toxicol (Phila). 2013. PMID: 23697460 Review.
References
-
- Brogan T.V., Lequier L., MacLaren G., Lorusso R., Peek G.J., Brodie D., Thiagarajan R., Vercaemst L. Extracorporeal Life Support: The ELSO Red Book. 6th ed. Extracorporeal Life Support Organization; Ann Arbor, MI, USA: 2022.
-
- Lindén V., Palmér K., Reinhard J., Westman R., Ehrén H., Granholm T., Frenckner B. High survival in adult patients with acute respiratory distress syndrome treated by extracorporeal membrane oxygenation, minimal sedation, and pressure supported ventilation. Intensive Care Med. 2000;26:1630–1637. doi: 10.1007/s001340000697. - DOI - PMC - PubMed
-
- Cucchi M., Mariani S., De Piero M.E., Ravaux J.M., Kawczynski M.J., Di Mauro M., Shkurka E., Hoskote A., Lorusso R. Awake extracorporeal life support and physiotherapy in adult patients: A systematic review of the literature. Perfusion. 2022;38:939–958. doi: 10.1177/02676591221096078. - DOI - PMC - PubMed
-
- Conrad S.A., Broman L.M., Taccone F.S., Lorusso R., Malfertheiner M.V., Pappalardo F., Di Nardo M., Belliato M., Grazioli L., Barbaro R.P., et al. The Extracorporeal Life Support Organization Maastricht Treaty for Nomenclature in Extracorporeal Life Support. A Position Paper of the Extracorporeal Life Support Organization. Am. J. Respir. Crit. Care Med. 2018;198:447–451. doi: 10.1164/rccm.201710-2130CP. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
