Gait Event Detection and Travel Distance Using Waist-Worn Accelerometers across a Range of Speeds: Automated Approach
- PMID: 38400313
- PMCID: PMC10891633
- DOI: 10.3390/s24041155
Gait Event Detection and Travel Distance Using Waist-Worn Accelerometers across a Range of Speeds: Automated Approach
Abstract
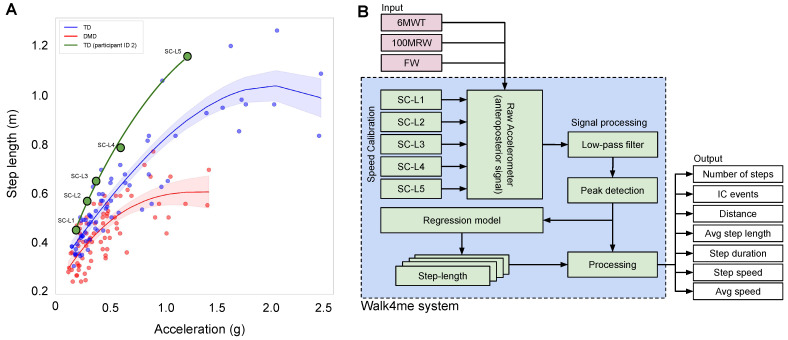
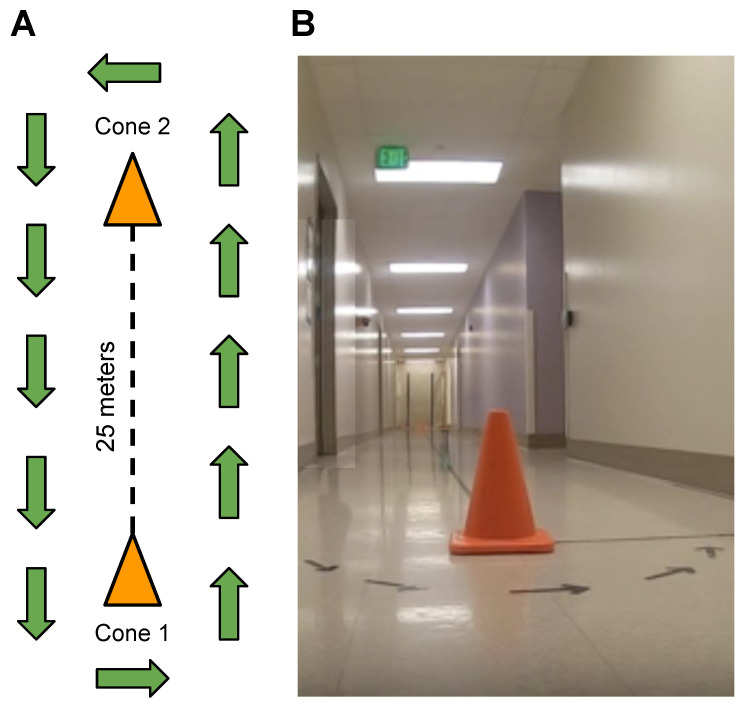
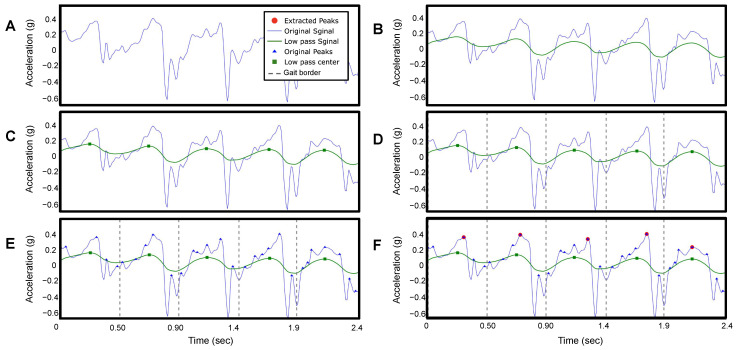
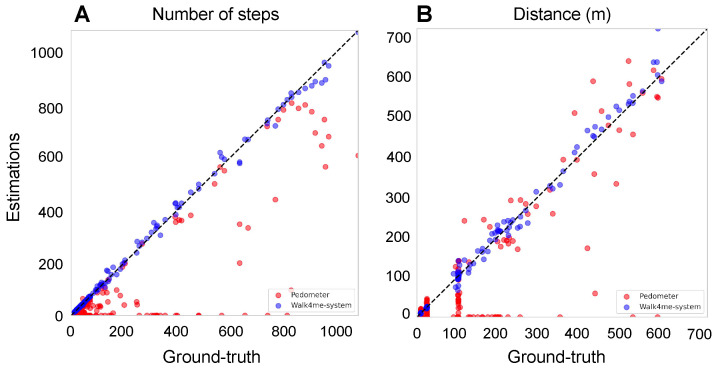
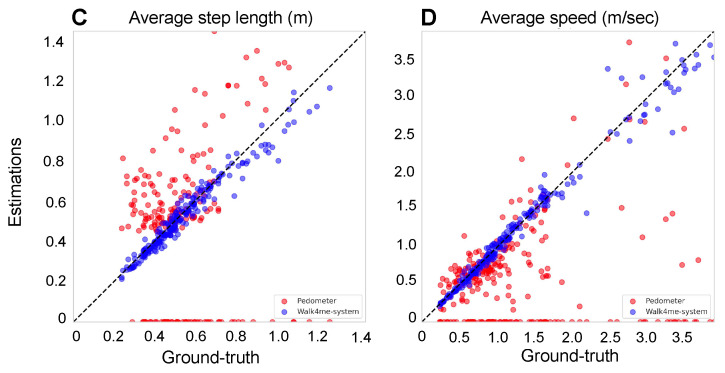
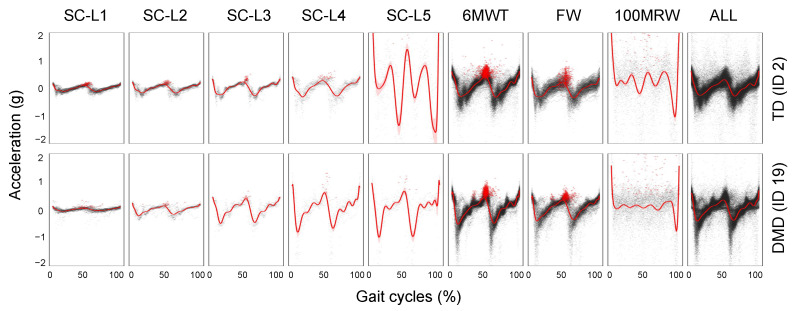
Estimation of temporospatial clinical features of gait (CFs), such as step count and length, step duration, step frequency, gait speed, and distance traveled, is an important component of community-based mobility evaluation using wearable accelerometers. However, accurate unsupervised computerized measurement of CFs of individuals with Duchenne muscular dystrophy (DMD) who have progressive loss of ambulatory mobility is difficult due to differences in patterns and magnitudes of acceleration across their range of attainable gait velocities. This paper proposes a novel calibration method. It aims to detect steps, estimate stride lengths, and determine travel distance. The approach involves a combination of clinical observation, machine-learning-based step detection, and regression-based stride length prediction. The method demonstrates high accuracy in children with DMD and typically developing controls (TDs) regardless of the participant's level of ability. Fifteen children with DMD and fifteen TDs underwent supervised clinical testing across a range of gait speeds using 10 m or 25 m run/walk (10 MRW, 25 MRW), 100 m run/walk (100 MRW), 6-min walk (6 MWT), and free-walk (FW) evaluations while wearing a mobile-phone-based accelerometer at the waist near the body's center of mass. Following calibration by a trained clinical evaluator, CFs were extracted from the accelerometer data using a multi-step machine-learning-based process and the results were compared to ground-truth observation data. Model predictions vs. observed values for step counts, distance traveled, and step length showed a strong correlation (Pearson's r = -0.9929 to 0.9986, p < 0.0001). The estimates demonstrated a mean (SD) percentage error of 1.49% (7.04%) for step counts, 1.18% (9.91%) for distance traveled, and 0.37% (7.52%) for step length compared to ground-truth observations for the combined 6 MWT, 100 MRW, and FW tasks. Our study findings indicate that a single waist-worn accelerometer calibrated to an individual's stride characteristics using our methods accurately measures CFs and estimates travel distances across a common range of gait speeds in both DMD and TD peers.
Keywords: Duchenne muscular dystrophy; accelerometer; gait cycle; machine learning; temporospatial gait clinical features; typically developing.
Conflict of interest statement
The authors declare no conflict of interest.
Figures