

Risk of major adverse cardiovascular events and stroke associated with treatment with GLP-1 or the dual GIP/GLP-1 receptor agonist tirzepatide for type 2 diabetes: A systematic review and meta-analysis
- PMID: 38400569
- PMCID: PMC11418422
- DOI: 10.1177/23969873241234238
Risk of major adverse cardiovascular events and stroke associated with treatment with GLP-1 or the dual GIP/GLP-1 receptor agonist tirzepatide for type 2 diabetes: A systematic review and meta-analysis
Abstract
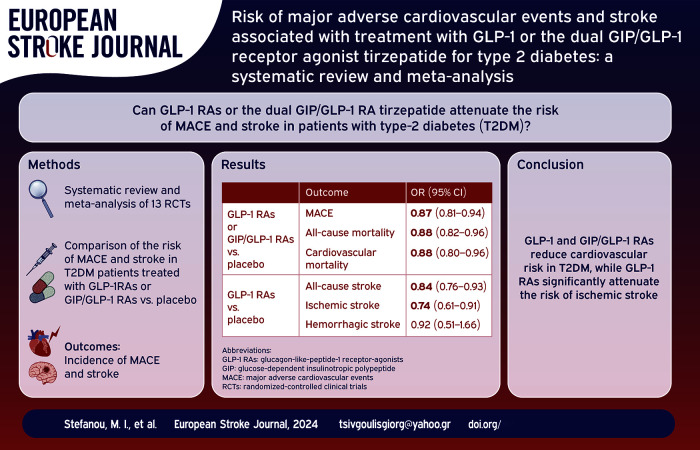
Introduction: Mounting evidence suggests that glucagon-like-peptide-1 receptor-agonists (GLP-1 RAs) attenuate cardiovascular-risk in type-2 diabetes (T2DM). Tirzepatide is the first-in-class, dual glucose-dependent-insulinotropic-polypeptide GIP/GLP-1 RA approved for T2DM.
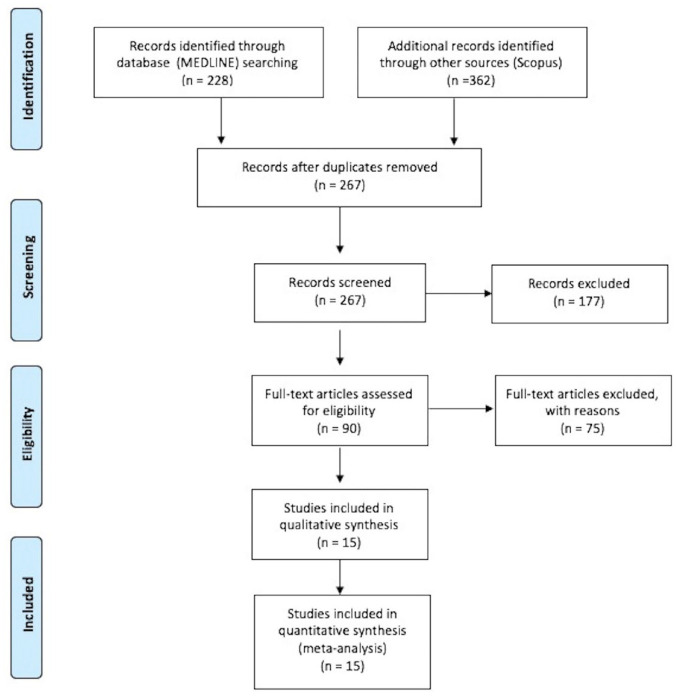
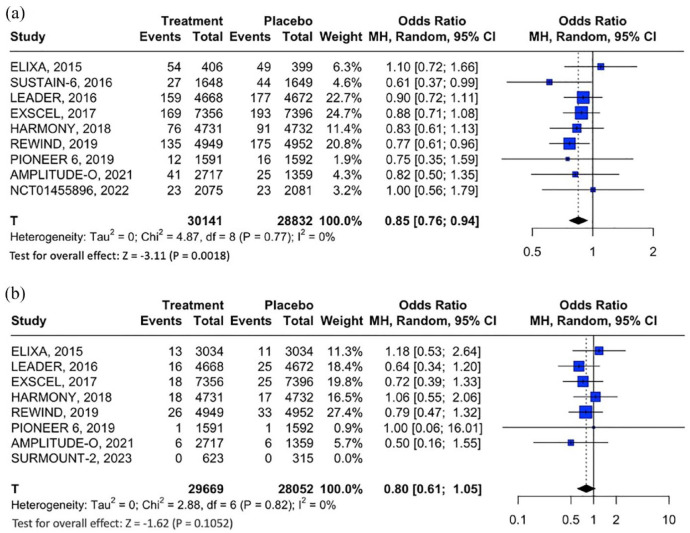
Patients and methods: A systematic review and meta-analysis of randomized-controlled clinical trials (RCTs) was performed to estimate: (i) the incidence of major adverse cardiovascular events (MACE); and (ii) incidence of stroke, fatal, and nonfatal stroke in T2DM-patients treated with GLP-1 or GIP/GLP-1 RAs (vs placebo).
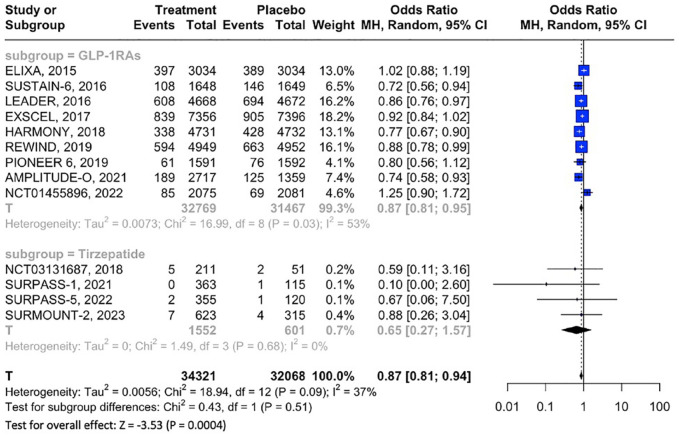
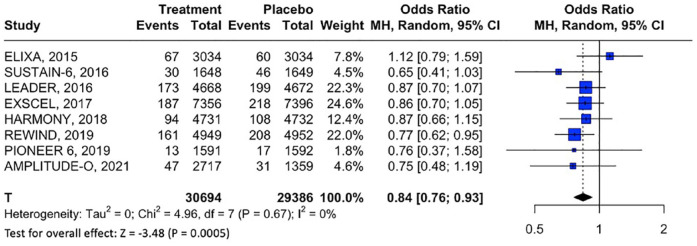
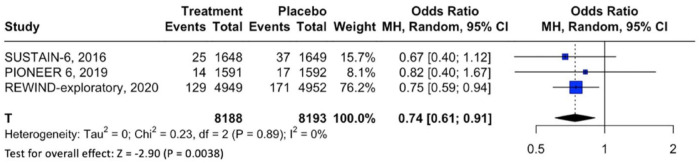
Results: Thirteen RCTs (9 and 4 on GLP-1 RAs and tirzepatide, respectively) comprising 65,878 T2DM patients were included. Compared to placebo, GLP-1RAs or GIP/GLP-1 RAs reduced MACE (OR: 0.87; 95% CI: 0.81-0.94; p < 0.01; I2 = 37%), all-cause mortality (OR: 0.88; 95% CI: 0.82-0.96; p < 0.01; I2 = 21%) and cardiovascular-mortality (OR: 0.88; 95% CI: 0.80-0.96; p < 0.01; I2 = 14%), without differences between GLP-1 versus GIP/GLP-1 RAs. Additionally, GLP-1 RAs reduced the odds of stroke (OR: 0.84; 95% CI: 0.76-0.93; p < 0.01; I2 = 0%) and nonfatal stroke (OR: 0.85; 95% CI: 0.76-0.94; p < 0.01; I2 = 0%), whereas no association between fatal stroke and GLP-1RAs was uncovered (OR: 0.80; 95% CI: 0.61-1.05; p = 0.105; I2 = 0%). In secondary analyses, GLP-1 RAs prevented ischemic stroke (OR: 0.74; 95% CI: 0.61-0.91; p < 0.01; I2 = 0%) and MACE-recurrence, but not hemorrhagic stroke (OR: 0.92; 95% CI: 0.51-1.66; p = 0.792; I2 = 0%). There was no association between GLP-1RAs or GIP/GLP-1 RAs and fatal or nonfatal myocardial infarction.
Discussion and conclusion: GLP-1 and GIP/GLP-1 RAs reduce cardiovascular-risk and mortality in T2DM. While there is solid evidence that GLP-1 RAs significantly attenuate the risk of ischemic stroke in T2DM, dedicated RCTs are needed to evaluate the efficacy of novel GIP/GLP-1 RAs for primary and secondary stroke prevention.
Keywords: GIP/GLP-1 receptor agonist; GLP-1; MACE; stroke; tirzepatide.
Conflict of interest statement
Declaration of conflicting interestsThe author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Khan MS, Fonarow GC, McGuire DK, et al. Glucagon-like peptide 1 receptor agonists and heart failure: the need for further evidence generation and practice guidelines optimization. Circulation 2020; 142: 1205–1218. - PubMed
-
- Kielgast U, Holst JJ, Madsbad S. Treatment of type 1 diabetic patients with glucagon-like peptide-1 (GLP-1) and GLP-1R agonists. Curr Diabetes Rev 2009; 5: 266–275. - PubMed
-
- Marx N, Husain M, Lehrke M, et al. GLP-1 receptor agonists for the reduction of atherosclerotic cardiovascular risk in patients with type 2 diabetes. Circulation 2022; 146: 1882–1894. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
