

Neighborhood social vulnerability and disparities in time to kidney cancer surgical treatment and survival in Arizona
- PMID: 38400688
- PMCID: PMC10891465
- DOI: 10.1002/cam4.7007
Neighborhood social vulnerability and disparities in time to kidney cancer surgical treatment and survival in Arizona
Abstract
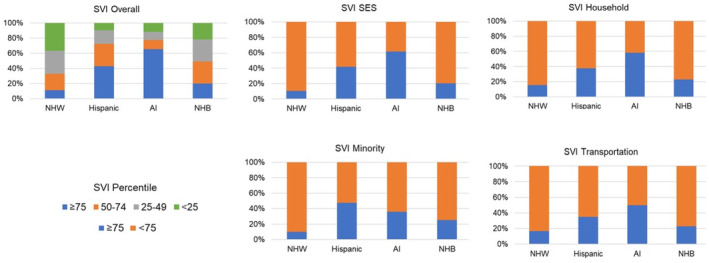
Background: Hispanics and American Indians (AI) have high kidney cancer incidence and mortality rates in Arizona. This study assessed: (1) whether racial and ethnic minority patients and patients from neighborhoods with high social vulnerability index (SVI) experience a longer time to surgery after clinical diagnosis, and (2) whether time to surgery, race and ethnicity, and SVI are associated with upstaging to pT3/pT4, disease-free survival (DFS), and overall survival (OS).
Methods: Arizona Cancer Registry (2009-2018) kidney and renal pelvis cases (n = 4592) were analyzed using logistic regression models to assess longer time to surgery and upstaging. Cox-regression hazard models were used to test DFS and OS.
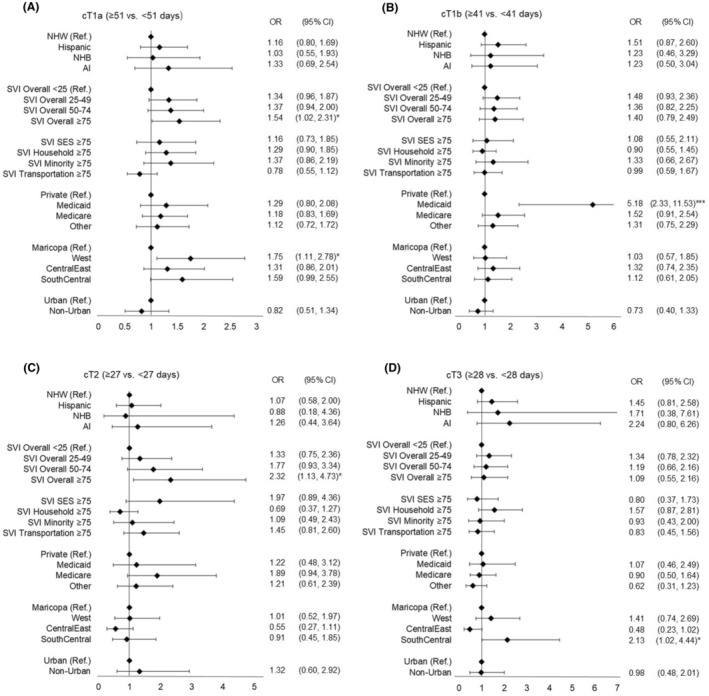
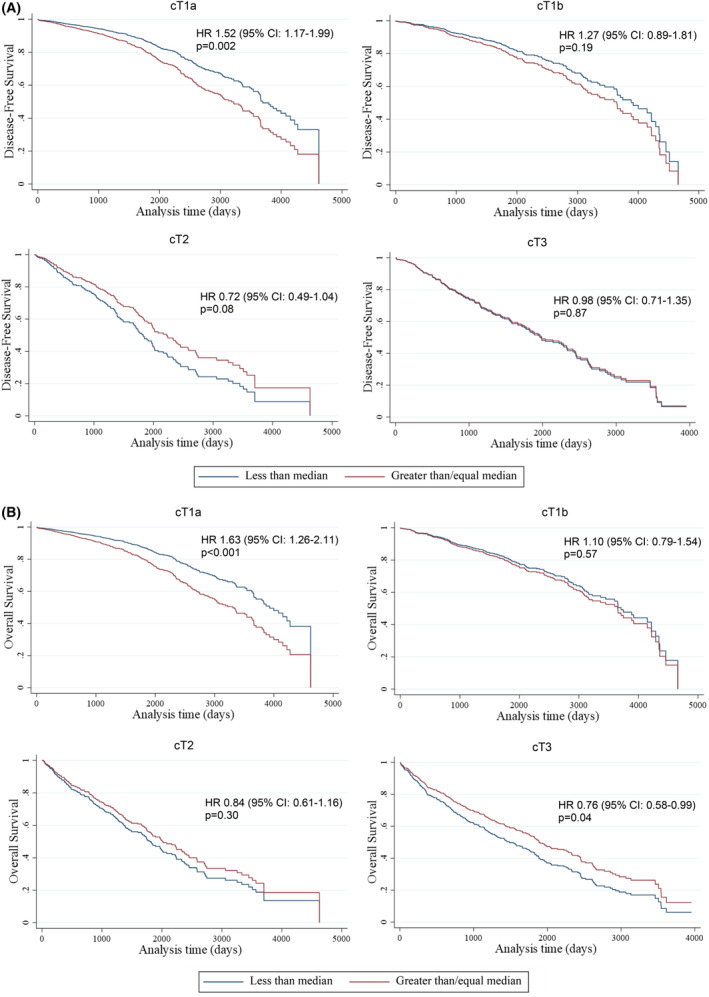
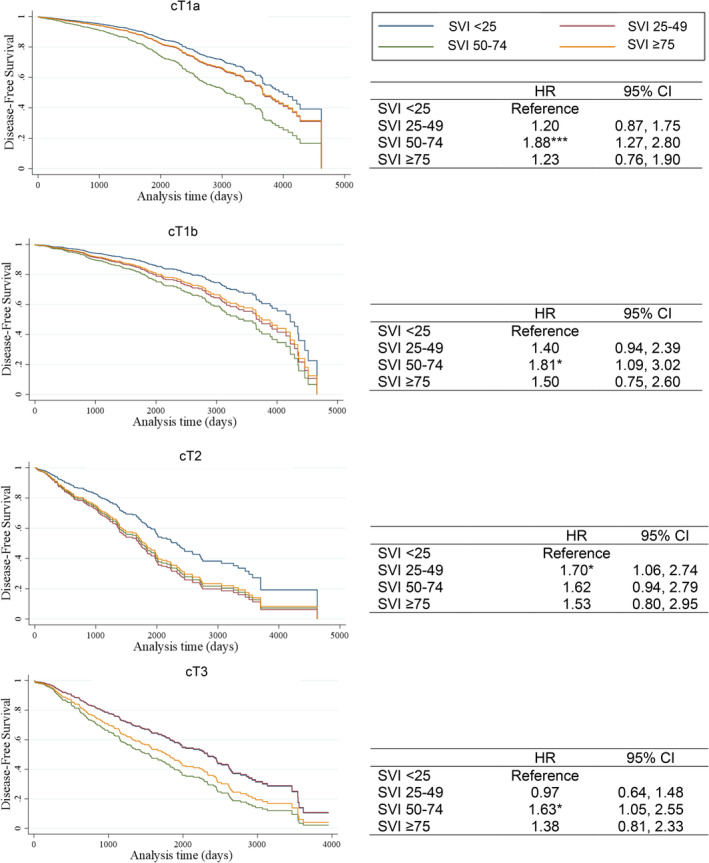
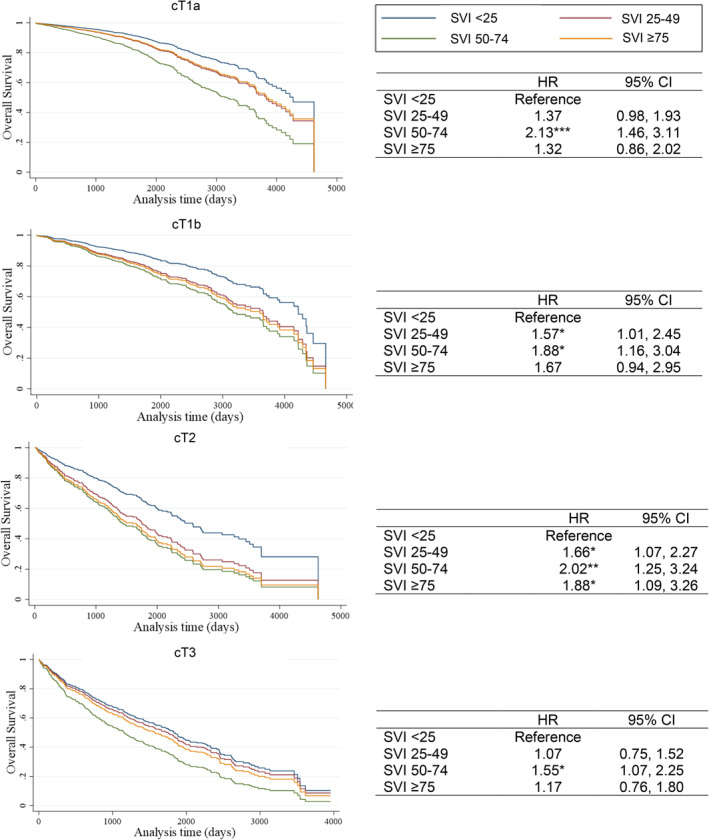
Results: Hispanic and AI patients with T1 tumors had a longer time to surgery than non-Hispanic White patients (median time of 56, 55, and 45 days, respectively). Living in neighborhoods with high (≥75) overall SVI increased odds of a longer time to surgery for cT1a (OR 1.54, 95% CI: 1.02-2.31) and cT2 (OR 2.32, 95% CI: 1.13-4.73). Race and ethnicity were not associated with time to surgery. Among cT1a patients, a longer time to surgery increased odds of upstaging to pT3/pT4 (OR 1.95, 95% CI: 0.99-3.84). A longer time to surgery was associated with PFS (HR 1.52, 95% CI: 1.17-1.99) and OS (HR 1.63, 95% CI: 1.26-2.11). Among patients with cT2 tumor, living in high SVI neighborhoods was associated with worse OS (HR 1.66, 95% CI: 1.07-2.57).
Conclusions: High social vulnerability was associated with increased time to surgery and poor survival after surgery.
Keywords: cancer health disparities; neighborhood factors; renal cancer; social determinants of health; treatment disparities.
© 2024 The Authors. Cancer Medicine published by John Wiley & Sons Ltd.
Conflict of interest statement
Dr Garcia is a National Board member for the American Cancer Society Cancer Action Network (CAN). The work here does not represent the views of the ACS CAN, and is not directly related to this manuscript.
Figures
Similar articles
-
Renal Cell Carcinoma Surgical Treatment Disparities in American Indian/Alaska Natives and Hispanic Americans in Arizona.Int J Environ Res Public Health. 2022 Jan 21;19(3):1185. doi: 10.3390/ijerph19031185. Int J Environ Res Public Health. 2022. PMID: 35162208 Free PMC article.
-
Impacts of Neighborhood Characteristics and Surgical Treatment Disparities on Overall Mortality in Stage I Renal Cell Carcinoma Patients.Int J Environ Res Public Health. 2022 Feb 12;19(4):2050. doi: 10.3390/ijerph19042050. Int J Environ Res Public Health. 2022. PMID: 35206240 Free PMC article.
-
Relationship of neighborhood social determinants of health on racial/ethnic mortality disparities in US veterans-Mediation and moderating effects.Health Serv Res. 2020 Oct;55 Suppl 2(Suppl 2):851-862. doi: 10.1111/1475-6773.13547. Epub 2020 Aug 29. Health Serv Res. 2020. PMID: 32860253 Free PMC article.
-
Inclusion of Race and Ethnicity With Neighborhood Socioeconomic Deprivation When Assessing COVID-19 Hospitalization Risk Among California Veterans Health Administration Users.JAMA Netw Open. 2023 Mar 1;6(3):e231471. doi: 10.1001/jamanetworkopen.2023.1471. JAMA Netw Open. 2023. PMID: 36867407 Free PMC article.
-
The impact of social vulnerability subthemes on postoperative outcomes differs by racial/ethnic minority status.Am J Surg. 2022 Feb;223(2):353-359. doi: 10.1016/j.amjsurg.2021.05.014. Epub 2021 Jun 1. Am J Surg. 2022. PMID: 34099239
References
-
- Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer statistics, 2023. CA Cancer J Clin. 2023;73:17‐48. - PubMed
-
- Palumbo C, Pecoraro A, Knipper S, et al. Contemporary age‐adjusted incidence and mortality rates of renal cell carcinoma: analysis according to gender, race, stage, grade, and histology. Eur Urol Focus. 2021;7:644‐652. - PubMed
-
- Bukavina L, Bensalah K, Bray F, et al. Epidemiology of renal cell carcinoma: 2022 update. Eur Urol. 2022;82:529‐542. - PubMed
-
- Escudier B, Porta C, Schmidinger M, et al. Renal cell carcinoma: ESMO clinical practice guidelines for diagnosis, treatment and follow‐up†. Ann Oncol. 2019;30:706‐720. - PubMed
-
- Ljungberg B, Albiges L, Abu‐Ghanem Y, et al. European Association of Urology guidelines on renal cell carcinoma: the 2022 update. Eur Urol. 2022;82:399‐410. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
