

COVID-19 and Influenza Vaccine Coadministration Among Older U.S. Adults
- PMID: 38401746
- PMCID: PMC11193626
- DOI: 10.1016/j.amepre.2024.02.013
COVID-19 and Influenza Vaccine Coadministration Among Older U.S. Adults
Abstract
Introduction: Coadministering COVID-19 and influenza vaccines is recommended by public health authorities and intended to improve uptake and convenience; however, the extent of vaccine coadministration is largely unknown. Investigations into COVID-19 and influenza vaccine coadministration are needed to describe compliance with newer recommendations and to identify potential gaps in the implementation of coadministration.
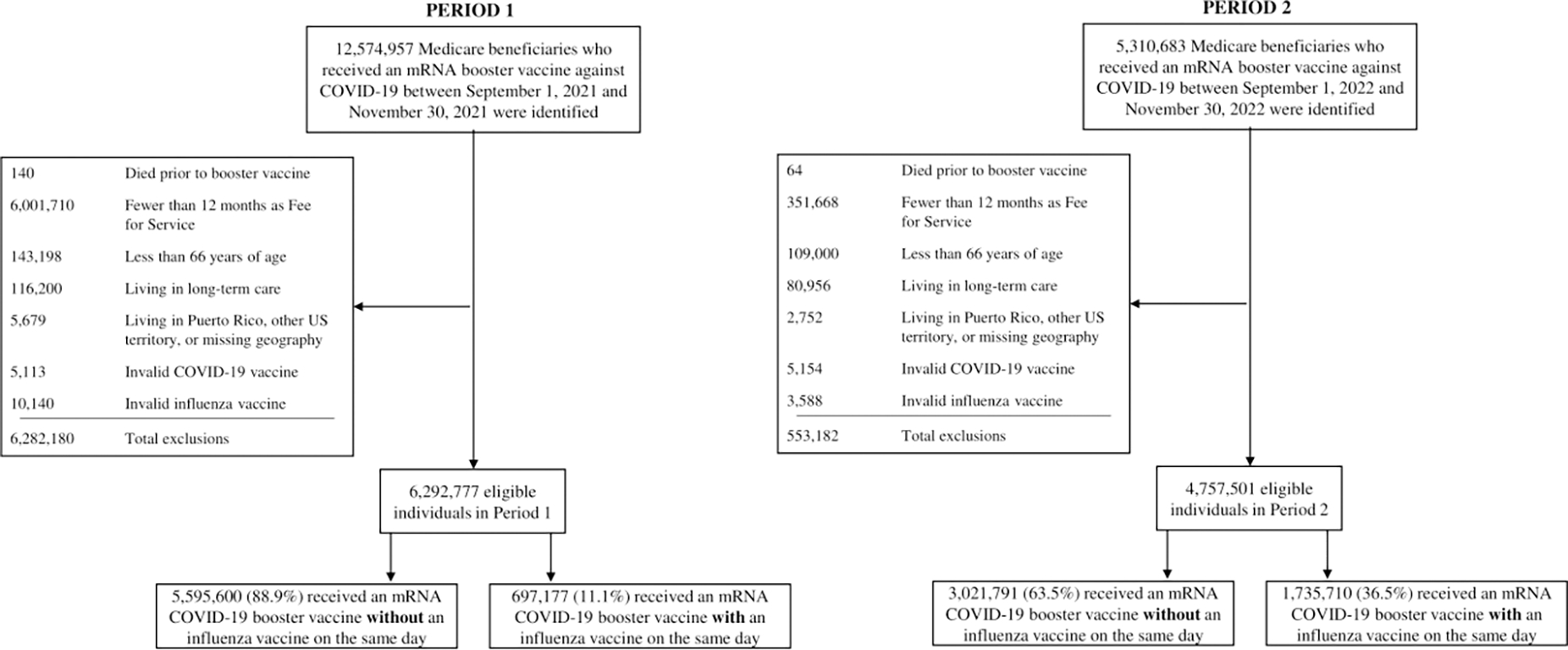
Methods: A descriptive, repeated cross-sectional study between September 1, 2021 to November 30, 2021 (Period 1) and September 1, 2022 to November 30, 2022 (Period 2) was conducted. This study included community-dwelling Medicare beneficiaries ≥ 66 years who received an mRNA COVID-19 booster vaccine in Periods 1 and 2. The outcome was an influenza vaccine administered on the same day as the COVID-19 vaccine. Adjusted ORs and 99% CIs were estimated using logistic regression to describe the association between beneficiaries' characteristics and vaccine coadministration. Statistical analysis was performed in 2023.
Results: Among beneficiaries who received a COVID-19 vaccine, 78.8% in Period 1 (N=6,292,777) and 89.1% in Period 2 (N=4,757,501), received an influenza vaccine at some point during the study period (i.e., before, after, or on the same day as their COVID-19 vaccine), though rates were lower in non-White and rural individuals. Vaccine coadministration increased from 11.1% to 36.5% between periods. Beneficiaries with dementia (aORPeriod 2=1.31; 99%CI=1.29-1.32) and in rural counties (aORPeriod 2=1.19; 99%CI=1.17-1.20) were more likely to receive coadministered vaccines, while those with cancer (aORPeriod 2=0.90; 99%CI=0.89-0.91) were less likely.
Conclusions: Among Medicare beneficiaries vaccinated against COVID-19, influenza vaccination was high, but coadministration of the 2 vaccines was low. Future work should explore which factors explain variation in the decision to receive coadministered vaccines.
Copyright © 2024 The Authors. Published by Elsevier Inc. All rights reserved.
Figures

References
-
- Benefits of Flu Vaccination During 2021–2022 Flu Season. Centers for Disease Control and Prevention. Published January 25, 2023. Accessed June 28, 2023. https://www.cdc.gov/flu/about/burden-averted/2021-2022.htm
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
