

Ultrasonic microbubbles promote mesenchymal stem cell homing to the fibrotic liver via upregulation of CXCR4 expression
- PMID: 38402155
- PMCID: PMC10894490
- DOI: 10.1186/s13008-023-00104-8
Ultrasonic microbubbles promote mesenchymal stem cell homing to the fibrotic liver via upregulation of CXCR4 expression
Abstract
Objective: To investigate the mechanism of ultrasound microbubbles (UTMB) promoting stem cells homing to fibrotic liver.
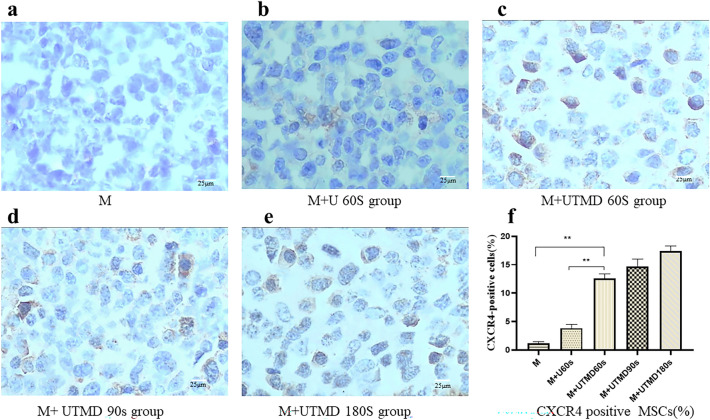
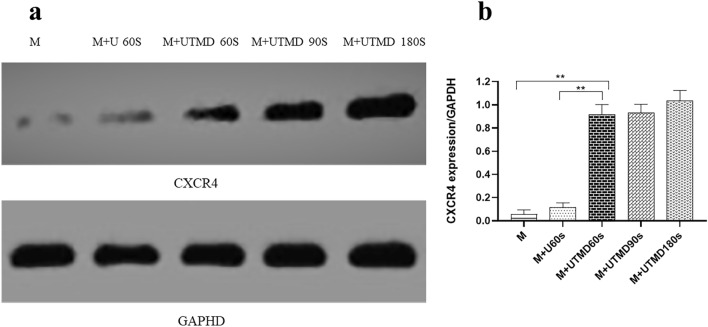
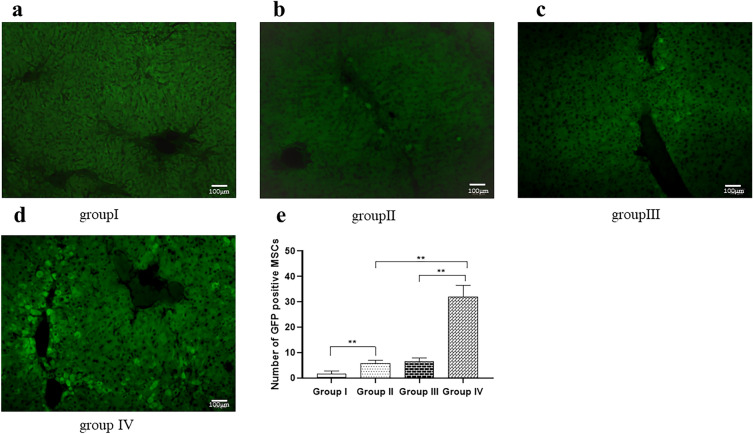
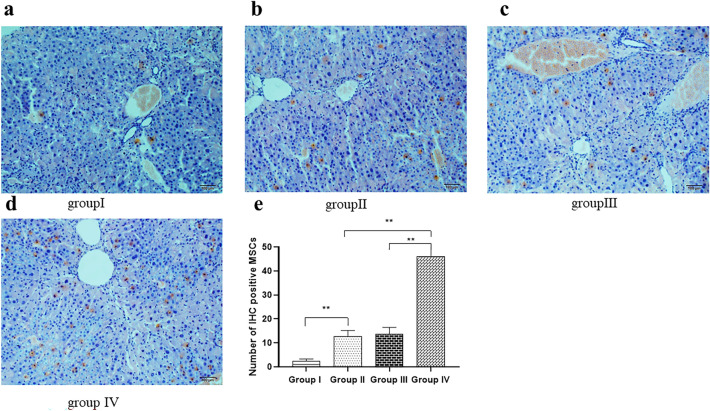
Methods: Bone marrow derived mesenchymal stem cells (BMSCs) were divided into 5 groups with or without ultrasound microbubbles and continuously irradiated with ultrasound conditions of frequency 1 MHZ and output power 0.6 W/cm2 for different times, and then injected into a mouse model of liver fibrosis through the tail vein with or without ultrasound microbubbles, with sound intensity. The effect of ultrasound microbubbles on MSC expression of CXC chemokine receptor 4 (CXCR4) and homing fibrotic liver was evaluated by flow cytometry (FCM), western blot (WB) and immunohistochemistry (IHC) analysis.
Results: The level of CXCR4 expression was significantly higher in the ultrasound microbubble group than in the non-intervention group (P < 0.05), and the number of MSC and the rate of CXCR4 receptor positivity in the ultrasound microbubble-treated liver tissues were significantly higher than in the non-intervention group (P < 0.01).
Conclusion: Ultrasonic microbubbles can promote the expression of CXCR4 on the surface of MSCs, thus improving the homing rate of MSCs in fibrotic liver.
Keywords: CXCR4; Homing; Liver fibrosis; Mesenchymal stem cell; Preface; Ultrasound microbubble.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



References
-
- Fang XQ, Liu LW, Dong J, et al. A study about immunomodulatory effect and efficacy and prognosis of human umbilical cord mesenchymal stem cells in patients with chronic hepatitis B-induced decompensated liver cirrhosis. J Gastroenterol Hepatol. 2018;33(4):774–780. doi: 10.1111/jgh.14081. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
