

Intestinal microbiota composition of children with glycogen storage Type I patients
- PMID: 38402355
- PMCID: PMC11078752
- DOI: 10.1038/s41430-024-01412-0
Intestinal microbiota composition of children with glycogen storage Type I patients
Erratum in
-
Correction: Intestinal microbiota composition of children with glycogen storage Type I patients.Eur J Clin Nutr. 2025 Mar;79(2):176. doi: 10.1038/s41430-024-01533-6. Eur J Clin Nutr. 2025. PMID: 39482381 Free PMC article. No abstract available.
Abstract
Aim: Dietary therapy of glycogen storage disease I (GSD I) is based on frequent feeding, with a high intake of complex carbohydrates (supplied by uncooked cornstarch), restriction of sugars, and a lower amount of lipids. There is limited information about the dietary regimen in patients with GSD, which might affect the intestinal luminal pH and microbiota composition. The aim of this study to investigate the intestinal microbiota composition in patients with GSD receiving diet treatment.
Method: Twelve patients who were followed up with GSD I after the diagnosis receiving diet therapy and 11 healthy children have been enrolled. Intestinal microbiota composition was evaluated by 16 s rRNA gene sequencing.
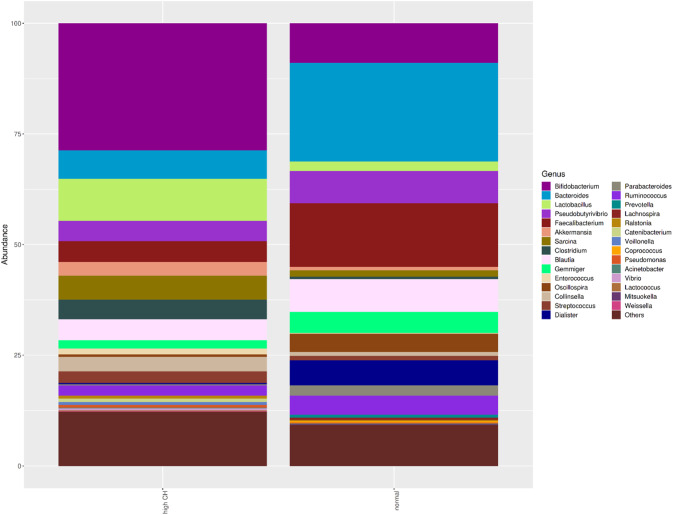
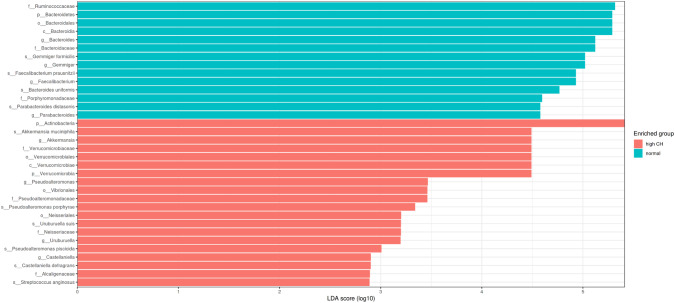
Results: A significant difference was found for beta-diversity between the GSD group and controls. A significantly lower abundance of Firmicutes and higher abundance of Actinobacteria was found in GSD group compared to the controls. Akkermansia, Pseudoalteromonas, Uruburella, and Castellaniella were dominant in the GSD patients at the genus level, while Faecalibacterium, Bacterioides, Gemmiger, Parabacteroides in the control group. At species level, Faecalibacterium prausnitzii decreased, and Akkermansia muciniphila were dominant in children with GSD.
Discussion: There is a substantial change in the composition of the gut microbiota, reduction of F. prausnitzii and an increase of A. muciniphila in children with GSD receiving consumption of uncooked cornstarch. Alterations of the intestinal microbiota might be related with the disease itself or dietary restrictions in patients with GSD, however, in certain condition, dysbiosis can negatively affect the course and make it difficult to control the disease.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
