

Impact of different sequential triple oral combination therapies based selexipag on outcomes in pulmonary arterial hypertension
- PMID: 38402556
- PMCID: PMC10894617
- DOI: 10.1002/clc.24245
Impact of different sequential triple oral combination therapies based selexipag on outcomes in pulmonary arterial hypertension
Abstract
Background: While the GRIPHON study and others have confirmed the efficacy and safety of selexipag with single, dual, and initial triple combination therapy for patients with pulmonary arterial hypertension (PAH), multicenters studies concerning diverse triple oral combination therapies based on selexipag are limited.
Hypothesis: This study was conducted to evaluate the effects of various sequential triple oral combination therapies on PAH outcomes.
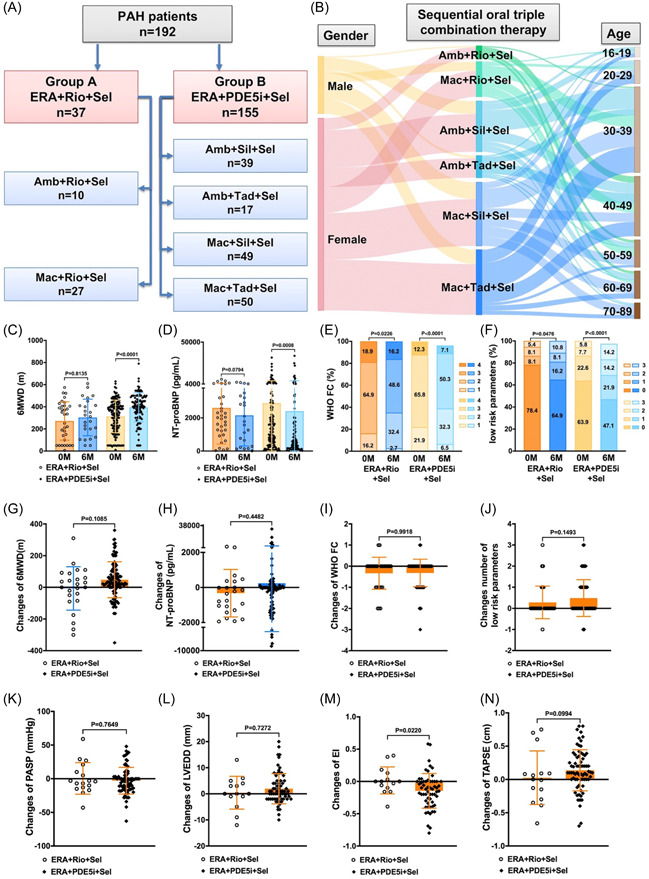
Methods: A retrospective study was carried out involving 192 patients from 10 centers, who were receiving sequential triple oral combination therapy consisting of an endothelin receptor antagonist (ERA), a phosphodiesterase 5 inhibitor (PDE5i)/riociguat and selexipag. Clinical parameters, event-free survival, and all-cause survival were assessed and analyzed at baseline and posttreatment.
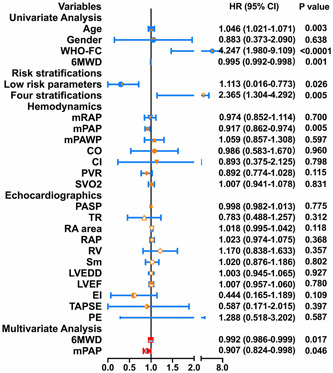
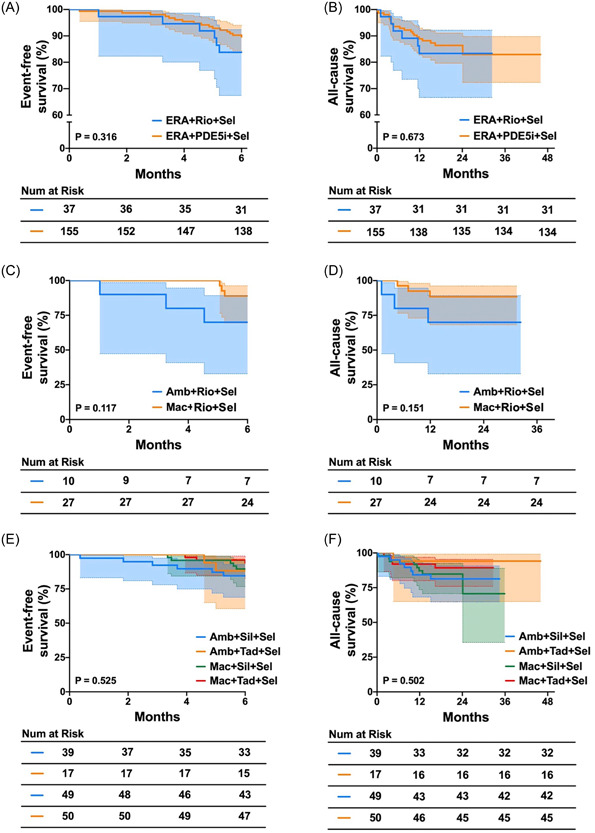
Results: Among the 192 patients, 37 were treated with ERA + riociguat + selexipag, and 155 patients received ERA + PDE5i + selexipag. Both sequential triple oral combination therapies improved the World Health Organization functional class and raised the count of low-risk parameters. As a result of the larger patients' population in the ERA + PDE5i + selexipag group, these individuals exhibited significant increases in 6-minute walking distance (6MWD), pulmonary arterial systolic pressure, pulmonary arterial pressure, right ventricle, and eccentricity index, and significant decreases in N-terminal probrain natriuretic peptide after 6 months of treatment. Nevertheless, both sequential triple oral combination therapy groups demonstrated similar shifts in these clinical parameters between baseline and 6 months. Baseline 6MWD and mean pulmonary arterial pressure were independent predictors of survival in patients undergoing ERA + PDE5i + selexipag therapy. Importantly, no significant differences were found in 6-month event-free survival and all-cause survival between two groups.
Conclusions: Different oral sequential triple combination therapies based on selexipag could comparably improve outcomes in patients with PAH.
Keywords: oral sequential triple combination therapy; pulmonary arterial hypertension; selexipag; survival.
© 2024 The Authors. Clinical Cardiology published by Wiley Periodicals, LLC.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Triple oral combination therapy with macitentan, riociguat, and selexipag for pulmonary arterial hypertension.Ther Adv Respir Dis. 2021 Jan-Dec;15:1753466621995048. doi: 10.1177/1753466621995048. Ther Adv Respir Dis. 2021. PMID: 33627044 Free PMC article.
-
Evaluating the efficacy and safety of oral triple sequential combination therapy for treating patients with pulmonary arterial hypertension: A multicenter retrospective study.Pulm Circ. 2024 Mar 10;14(1):e12351. doi: 10.1002/pul2.12351. eCollection 2024 Jan. Pulm Circ. 2024. PMID: 38468630 Free PMC article.
-
Real-Life Experience with Selexipag as an Add-On Therapy to Oral Combination Therapy in Patients with Pulmonary Arterial or Distal Chronic Thromboembolic Pulmonary Hypertension: A Retrospective Analysis.Lung. 2019 Jun;197(3):353-360. doi: 10.1007/s00408-019-00222-7. Epub 2019 Apr 8. Lung. 2019. PMID: 30963265
-
Selexipag for the treatment of pulmonary arterial hypertension.Expert Rev Respir Med. 2021 May;15(5):583-595. doi: 10.1080/17476348.2021.1866990. Epub 2020 Dec 31. Expert Rev Respir Med. 2021. PMID: 33382345 Review.
-
A Special Focus on Selexipag - Treatment of Pulmonary Arterial Hypertension.Curr Pharm Des. 2017;23(34):5191-5199. doi: 10.2174/1381612823666170908114227. Curr Pharm Des. 2017. PMID: 28891448 Review.
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
