

Noninvasive Electromagnetic Phrenic Nerve Stimulation in Critically Ill Patients: A Feasibility Study
- PMID: 38403186
- PMCID: PMC11443241
- DOI: 10.1016/j.chest.2024.02.035
Noninvasive Electromagnetic Phrenic Nerve Stimulation in Critically Ill Patients: A Feasibility Study
Abstract
Background: Electromagnetic stimulation of the phrenic nerve induces diaphragm contractions, but no coils for clinical use have been available. We recently demonstrated the feasibility of ventilation using bilateral transcutaneous noninvasive electromagnetic phrenic nerve stimulation (NEPNS) before surgery in lung-healthy patients with healthy weight in a dose-dependent manner.
Research question: Is NEPNS feasible in critically ill patients in an ICU setting?
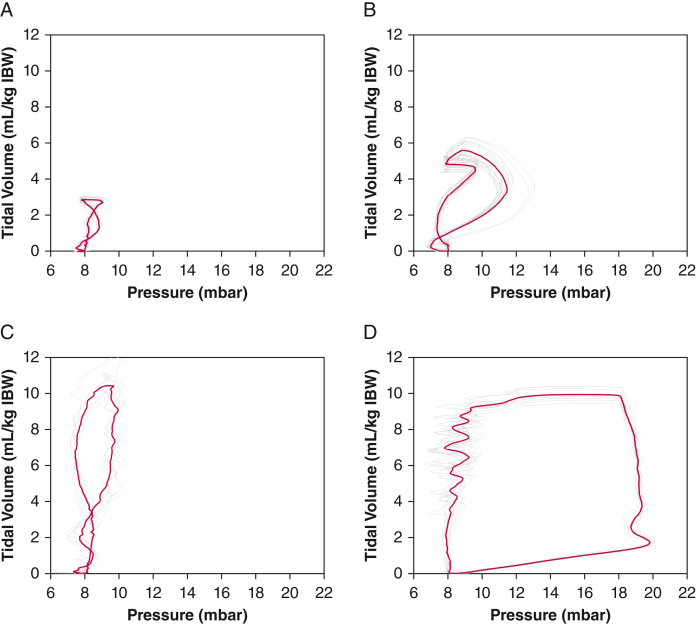
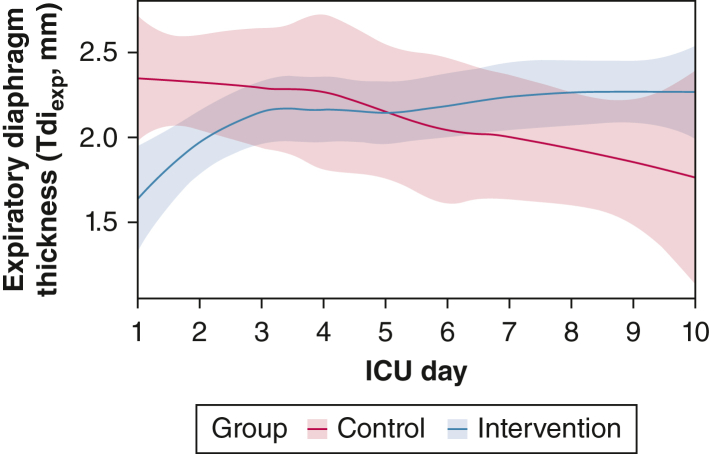
Study design and methods: This feasibility nonrandomized controlled study aimed to enroll patients within 36 h of intubation who were expected to remain ventilated for ≥ 72 h. The intervention group received 15-min bilateral transcutaneous NEPNS bid, whereas the control group received standard care. If sufficient, NEPNS was used without pressure support to ventilate the patient; pressure support was added if necessary to ventilate the patient adequately. The primary outcome was feasibility, measured as time to find the optimal stimulation position. Further end points were sessions performed according to the protocol or allowing a next-day catch-up session and tidal volume achieved with stimulation reaching only 3 to 6 mL/kg ideal body weight (IBW). A secondary end point was expiratory diaphragm thickness measured with ultrasound from days 1 to 10 (or extubation).
Results: The revised European Union regulation mandated reapproval of medical devices, prematurely halting the study. Eleven patients (five in the intervention group, six in the control group) were enrolled. The median time to find an adequate stimulation position was 23 s (interquartile range, 12-62 s). The intervention bid was executed in 87% of patients, and 92% of patients including a next-day catch-up session. Ventilation with 3 to 6 mL/kg IBW was achieved in 732 of 1,701 stimulations (43.0%) with stimulation only and in 2,511 of 4,036 stimulations (62.2%) with additional pressure support. A decrease in diaphragm thickness was prevented by bilateral NEPNS (P = .034) until day 10.
Interpretation: Bilateral transcutaneous NEPNS was feasible in the ICU setting with the potential benefit of preventing diaphragm atrophy during mechanical ventilation. NEPNS ventilation effectiveness needs further assessment.
Trial registry: ClinicalTrials.gov; No.: NCT05238753; URL: www.
Clinicaltrials: gov.
Keywords: ICUs; artificial; critical care; critical illness; interactive ventilatory support; magnetic field therapy; magnetic fields; magnetic stimulation therapy; muscular atrophy; respiration; ventilator weaning.
Copyright © 2024 The Author(s). Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Financial/Nonfinancial Disclosures The authors have reported to CHEST the following: S. J. S. reports grants and nonfinancial support from STIMIT AG for this work, grants and nonfinancial support from Reactive Robotics GmbH, ASP GmbH, and ESICM; grants, personal fees, and nonfinancial support from Fresenius Kabi Deutschland GmbH; grants from the Innovationsfond of The Federal Joint Committee (G-BA); personal fees from Springer Verlag GmbH for educational purposes and Advanz Pharma GmbH; and nonfinancial support from national and international societies (and their congress organizers) in the field of anesthesiology and intensive care medicine, outside the submitted work; holds stocks in small amounts from Alphabeth, Inc., Bayer AG, and Siemens AG; these holdings have not affected any decisions regarding his research or this study. A. P. holds stocks in small amounts from BioNTech SE, Taiwan Semiconductor, Sony, Pfizer, Arcutis Biotherapeutics, Inc., Sangamo Therapeutics, NIO, and Ke Holdings; these holdings have not affected any decisions regarding his research or this study. L. B. has received research grants from STIMIT, Medtronic, and Draeger and equipment from Sentec, Philips, and Fisher Paykel. None declared (A. M. G., S. K., M. A. V., B. U., J. J. G., H. G. B., N. M. C., T. N., S. W.-C.).
Figures
References
-
- Dot I., Pérez-Teran P., Samper M.-A., Masclans J.-R. Diaphragm dysfunction in mechanically ventilated patients. Arch Bronconeumol (Engl Ed) 2017;53(3):150–156. - PubMed
-
- Kilapong B., Aditianingsih D., Sedono R., Sugiarto A., Salamah T. Diaphragm muscle thinning in mechanically ventilated critically ill patients. J Pak Med Assoc. 2021;71(suppl 2):S78–S83. 2. - PubMed
-
- Levine S., Nguyen T., Taylor N., et al. Rapid disuse atrophy of diaphragm fibers in mechanically ventilated humans. N Engl J Med. 2008;358(13):1327–1335. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
