

Hereditary epidermolysis bullosa: clinical-epidemiological profile of 278 patients at a tertiary hospital in São Paulo, Brazil
- PMID: 38403552
- PMCID: PMC11074615
- DOI: 10.1016/j.abd.2023.06.009
Hereditary epidermolysis bullosa: clinical-epidemiological profile of 278 patients at a tertiary hospital in São Paulo, Brazil
Abstract
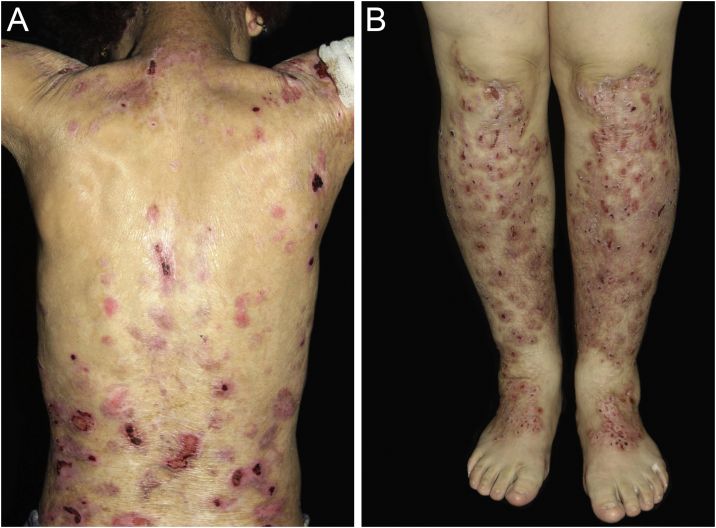
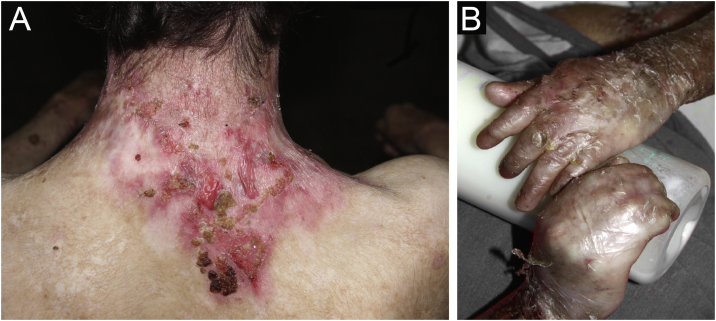
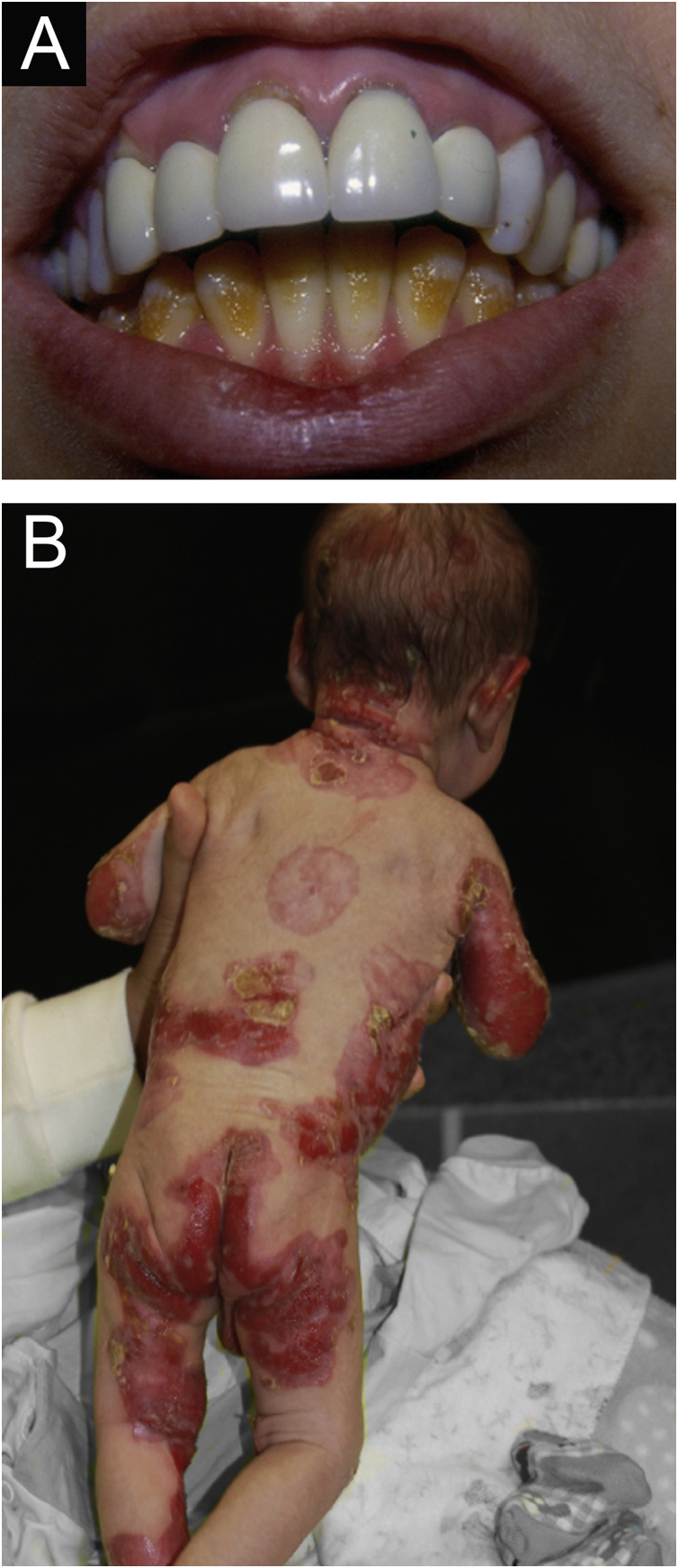
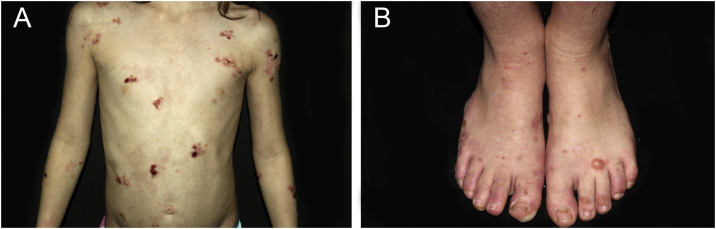
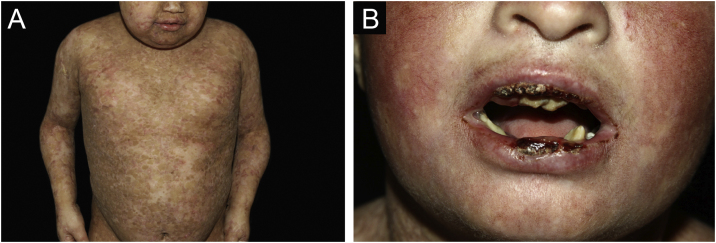
Background: Epidermolysis bullosa (EB) is a group of rare hereditary diseases, characterized by fragility of the skin and mucous membranes. Epidemiological data on EB in Brazil are scarce.
Objectives: To describe epidemiological aspects of patients with EB diagnosed in the Dermatology Department of a tertiary hospital, from 2000 to 2022.
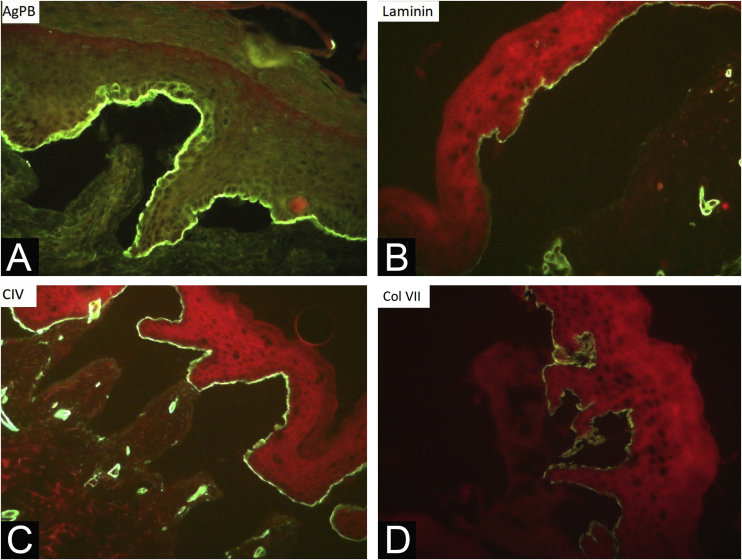
Methods: An observational and retrospective study was conducted through the analysis of medical records. The evaluated data included clinical form, sex, family history, consanguinity, age at diagnosis, current age, time of follow-up, comorbidities, histopathology and immunomapping, presence of EB nevi and squamous cell carcinomas (SCC), cause of and age at death.
Results: Of 309 patients with hereditary EB, 278 were included. The most common type was dystrophic EB (DEB), with 73% (28.4% dominant DEB, 31.7% recessive DEB and 12.9% pruriginous DEB). Other types were junctional EB with 9.4%, EB simplex with 16.5% and Kindler EB with 1.1%. Women accounted for 53% and men for 47% of cases. Family history was found in 35% and consanguinity in 11%. The mean age at diagnosis was 10.8 years and the current age was 26 years. The mean time of follow-up was nine years. Esophageal stenosis affected 14%, dental alterations affected 36%, malnutrition 13% and anemia 29%. During diagnostic investigation, 72.6% underwent histopathological examination and 92% underwent immunomapping. EB nevi were identified in 17%. Nine patients had SCC. Eleven patients died.
Study limitations: Insufficient data included to medical records, loss to follow-up, and unavailability of genetic testing.
Conclusions: In this study, dystrophic EB predominated and the need for multidisciplinary care for comorbidities and complications was highlighted.
Keywords: Brazil; Epidemiology; Epidermolysis bullosa; Epidermolysis bullosa dystrophica; Epidermolysis bullosa simplex; Epidermolysis bullosa, junctional; Tertiary healthcare.
Copyright © 2024 Sociedade Brasileira de Dermatologia. Published by Elsevier España, S.L.U. All rights reserved.
Figures

Similar articles
-
Assessment of the Timing of Milestone Clinical Events in Patients With Epidermolysis Bullosa From North America.JAMA Dermatol. 2019 Feb 1;155(2):196-203. doi: 10.1001/jamadermatol.2018.4673. JAMA Dermatol. 2019. PMID: 30586139 Free PMC article.
-
Advantages of whole-exome sequencing over immunomapping in 67 Brazilian patients with epidermolysis bullosa.An Bras Dermatol. 2024 May-Jun;99(3):350-356. doi: 10.1016/j.abd.2023.07.002. Epub 2024 Feb 16. An Bras Dermatol. 2024. PMID: 38368142 Free PMC article.
-
Multidisciplinary care for patients with epidermolysis bullosa from birth to adolescence: experience of one Italian reference center.Ital J Pediatr. 2022 Apr 12;48(1):58. doi: 10.1186/s13052-022-01252-3. Ital J Pediatr. 2022. PMID: 35414096 Free PMC article.
-
Inherited epidermolysis bullosa: epidemiology and patient care in Slovenia with a review of the updated classification.Acta Dermatovenerol Alp Pannonica Adriat. 2021 Jun;30(2):63-66. Acta Dermatovenerol Alp Pannonica Adriat. 2021. PMID: 34169701 Review.
-
Epidermolysis Bullosa: Pediatric Perspectives.Curr Pediatr Rev. 2022;18(3):182-190. doi: 10.2174/1573396317666210525161252. Curr Pediatr Rev. 2022. PMID: 34036913 Review.
Cited by
-
Paw Skin as a Translational Model for Investigating Fibrotic and Inflammatory Wound Healing Defects in Recessive Dystrophic Epidermolysis Bullosa.Int J Mol Sci. 2025 Apr 30;26(9):4281. doi: 10.3390/ijms26094281. Int J Mol Sci. 2025. PMID: 40362519 Free PMC article.
References
-
- Has C., Bauer J.W., Bodemer C., Bolling M.C., Bruckner-Tuderman L., Diem A., et al. Consensus reclassification of inherited epidermolysis bullosa and other disorders with skin fragility. Br J Dermatol. 2020;183:614–627. - PubMed
-
- Bardhan A., Bruckner-Tuderman L., Chapple I.L.C., Fine J.D., Harper N., Has C., et al. Epidermolysis bullosa. Nat Rev Dis Primers. 2020;6:78. - PubMed
-
- Mariath L.M., Santin J.T., Frantz J.A., Doriqui M.J.R., Kiszewski A.E., Schuler-Faccini L. An overview of the genetic basis of epidermolysis bullosa in Brazil: discovery of novel and recurrent disease-causing variants. Clin Genet. 2019;96:189–198. - PubMed
-
- Melo J.N., Teruya P.Y., Machado M.C., Valente N.S., Sotto M.N., Oliveira Z.N. Epidermolysis bullosa nevi: clinical, dermatoscopical and histological features in a case of recessive dystrofic form. An Bras Dermatol. 2011;86:743–746. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
