

Severe Left Main Coronary Artery Stenosis and Aortic Regurgitation in a Patient Presenting with Takayasu Arteritis
- PMID: 38403770
- PMCID: PMC11518588
- DOI: 10.2169/internalmedicine.3032-23
Severe Left Main Coronary Artery Stenosis and Aortic Regurgitation in a Patient Presenting with Takayasu Arteritis
Abstract
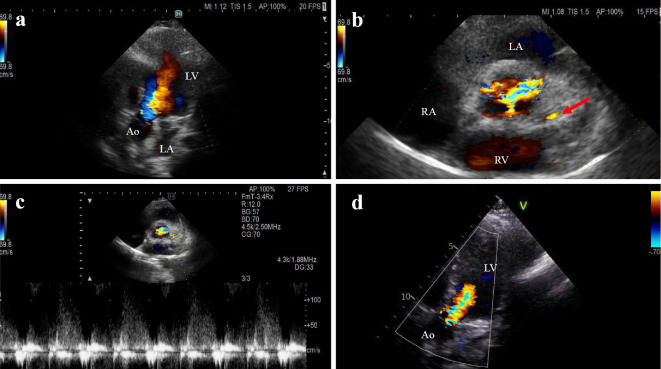
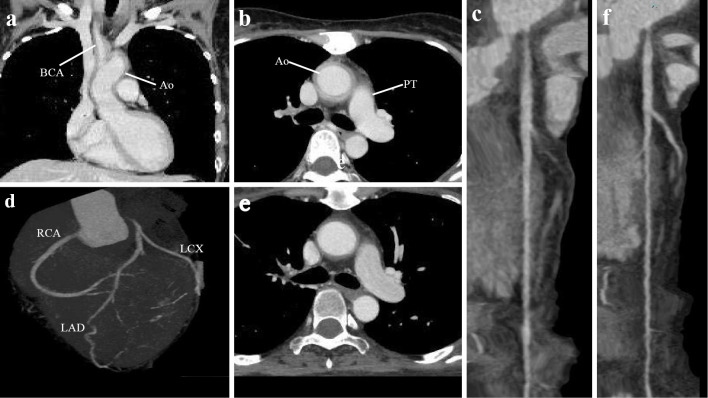
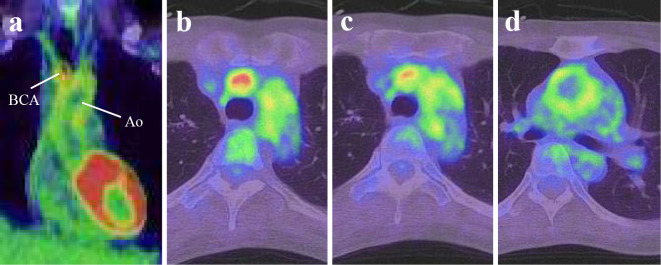
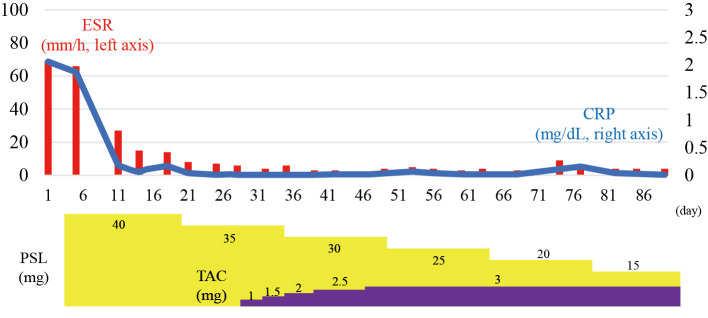
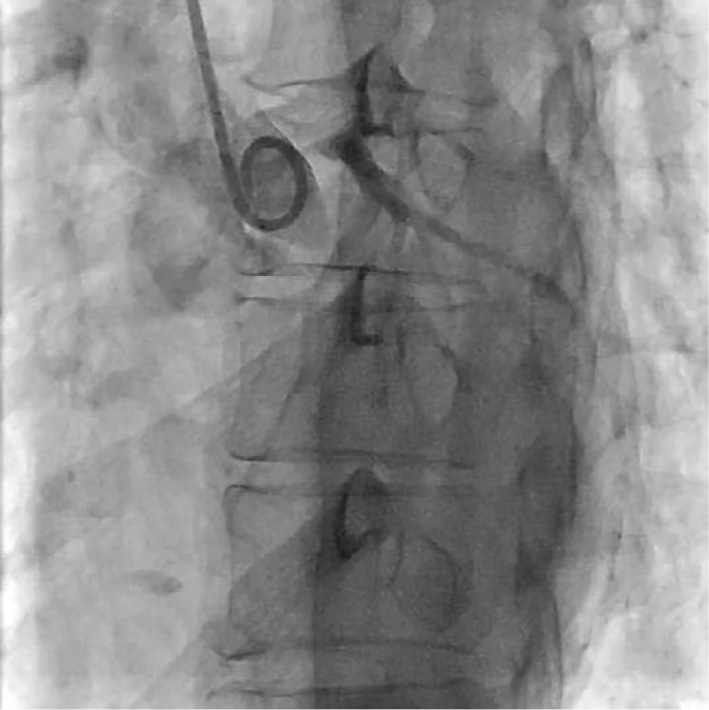
We herein report the case of a 46-year-old woman with Takayasu arteritis (TA), severe stenosis in the left main coronary artery (LMCA), and severe aortic regurgitation. Prednisolone and tacrolimus were initiated as TA treatments. Two months after initiating medical therapy, the aortic regurgitation severity improved to a moderate grade, although there was no obvious improvement in LMCA stenosis. Thus, after confirming the resolution of inflammation, we performed coronary artery bypass grafting alone without any aortic valve intervention. In TA patients with severe LMCA stenosis, surgical management of the coronary artery should therefore be considered only after successfully administering anti-inflammatory therapy.
Keywords: Takayasu arteritis; anti-inflammatory therapy; coronary artery bypass grafting; coronary artery disease.
Conflict of interest statement
Figures

Similar articles
-
Complete occlusion of the left main coronary artery ostium in Takayasu arteritis.J Thorac Cardiovasc Surg. 2008 Mar;135(3):695-6. doi: 10.1016/j.jtcvs.2007.11.031. J Thorac Cardiovasc Surg. 2008. PMID: 18329499 No abstract available.
-
Regressed coronary ostial stenosis in a young female with Takayasu arteritis: a case report.BMC Cardiovasc Disord. 2019 Apr 2;19(1):79. doi: 10.1186/s12872-019-1066-7. BMC Cardiovasc Disord. 2019. PMID: 30940076 Free PMC article.
-
Simultaneous repair of stenosis in coronary and vertebral arteries and aortic regurgitation secondary to Takayasu's aortitis.Jpn J Thorac Cardiovasc Surg. 2002 Feb;50(2):88-91. doi: 10.1007/BF02919672. Jpn J Thorac Cardiovasc Surg. 2002. PMID: 11905066
-
Surgical treatment of cardiac involvement in Takayasu arteritis.Heart Vessels Suppl. 1992;7:168-78. doi: 10.1007/BF01744564. Heart Vessels Suppl. 1992. PMID: 1360964 Review.
-
[Left coronary ostial stenosis and aortic regurgitation associated with syphilitic aortitis; report of a case].Kyobu Geka. 2010 Jul;63(7):590-3. Kyobu Geka. 2010. PMID: 20662242 Review. Japanese.
References
-
- Seyahi E. Takayasu arteritis: an update. Curr Opin Rheumatol 29: 51-56, 2017. - PubMed
-
- Isobe M, Amano K, Arimura Y, et al. .; the JCS Joint Working Group. JCS 2017 Guideline on Management of Vasculitis Syndrome - digest version. Circ J 84: 299-359, 2020. - PubMed
-
- Keser G, Aksu K, Direskeneli H. Takayasu arteritis: an update. Turk J Med Sci 48: 681-697, 2018. - PubMed
-
- Rav-Acha M, Plot L, Peled N, Amital H. Coronary involvement in Takayasu's arteritis. Autoimmun Rev 6: 566-571, 2007. - PubMed
-
- Endo M, Tomizawa Y, Nishida H, et al. . Angiographic findings and surgical treatments of coronary artery involvement in Takayasu arteritis. J Thorac Cardiovasc Surg 125: 570-577, 2003. - PubMed