

Myocarditis and COVID-19 related issues
- PMID: 38404624
- PMCID: PMC10886760
- DOI: 10.21542/gcsp.2023.28
Myocarditis and COVID-19 related issues
Abstract
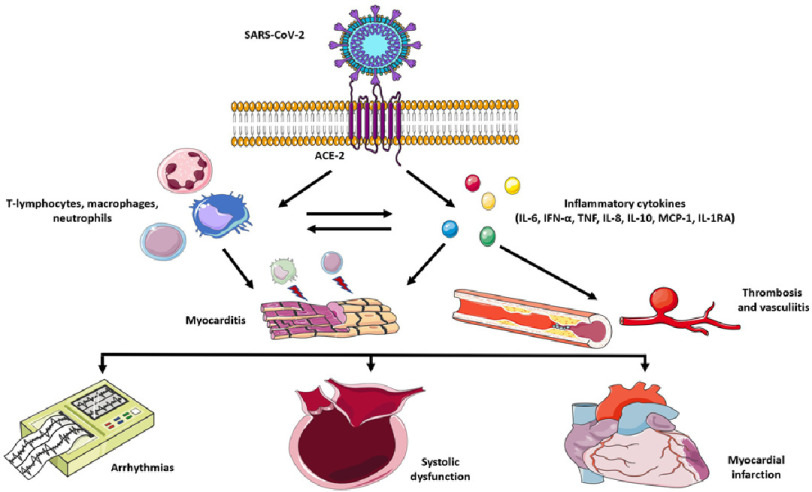
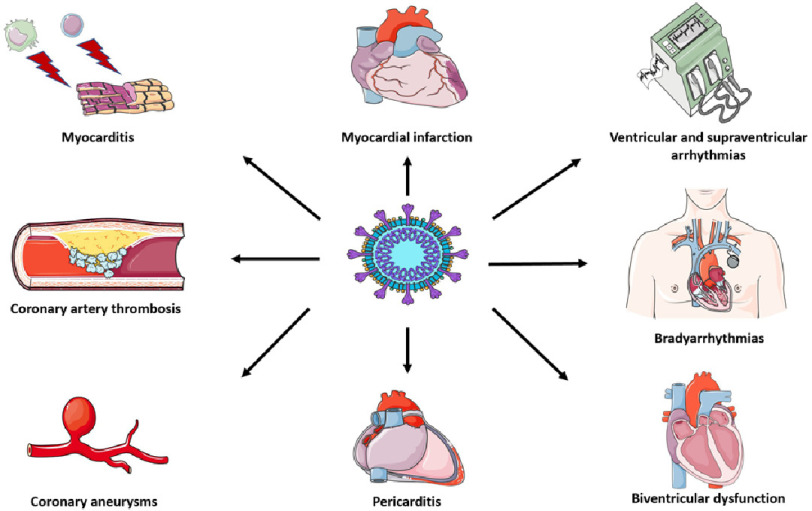
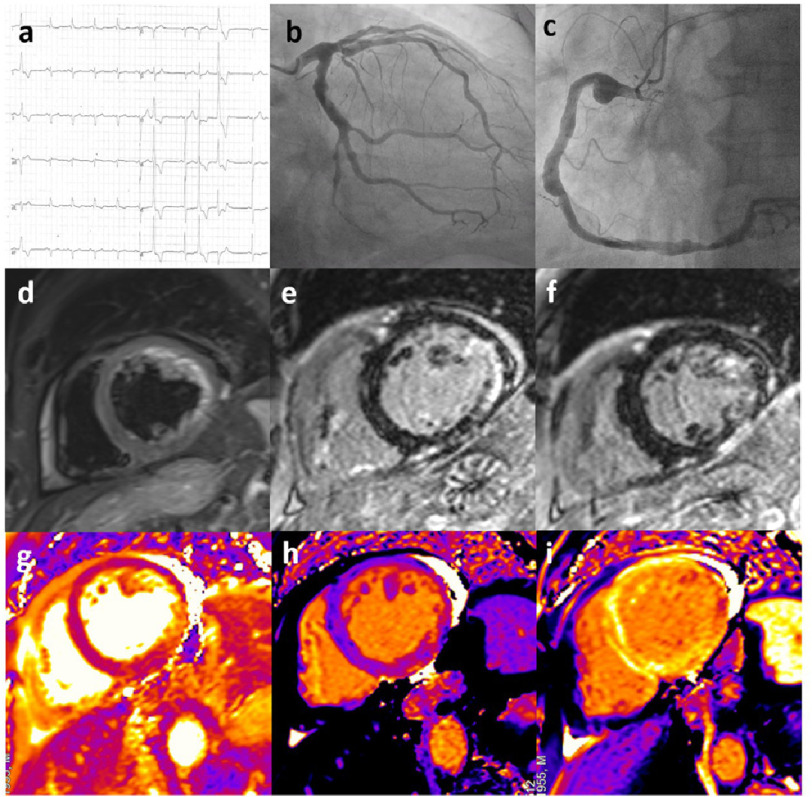
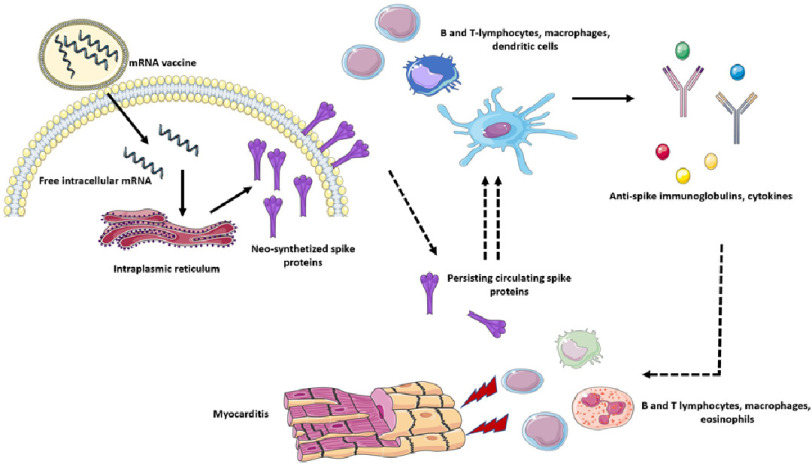
The recent COVID-19 (Coronavirus Disease 2019) pandemic by SARS-CoV2 infection has caused millions of deaths and hospitalizations across the globe. In the early pandemic phases, the infection had been initially considered a primary pulmonary disease. However, increasing evidence has demonstrated a wide range of possible cardiac involvement. Most of systemic and cardiac damage is likely sustained by a complex interplay between inflammatory, immune-related and thrombotic mechanisms. Biventricular failure and myocardial damage with elevation of cardiac biomarkers have been reported in COVID-19 patients, although histological demonstration of acute myocarditis has been rarely documented. Indeed while cardiac magnetic resonance findings include different patterns of myocardial involvement in terms of late gadolinium enhancement, histological data from necropsy and endomyocardial biopsy showed peculiar inflammatory patterns, mostly composed by macrophages. On the other hand COVID-19 vaccines based on mRN technology have been also associated with increased risk of myocarditis. COVID-19 and mRNA vaccine-related myocarditis present different clinical and imaging presentations and recent data suggest the presence of distinctive immunological mechanisms involved.
Copyright ©2023 The Author(s).
Figures
References
-
- Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z, Xiang J, Wang Y, Song B, Gu X, Guan L, Wei Y, Li H, Wu X, Xu J, Tu S, Zhang Y, Chen H, Cao B. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020;395(10229):1054–1062. - PMC - PubMed
-
- Kotecha T, Knight DS, Razvi Y, Kumar K, Vimalesvaran K, Thornton G, Patel R, Chacko L, Brown JT, Coyle C, Leith D, Shetye A, Ariff B, Bell R, Captur G, Coleman M, Goldring J, Gopalan D, Heightman M, Hillman T, Howard L, Jacobs M, Jeetley PS, Kanagaratnam P, Kon OM, Lamb LE, Manisty CH, Mathurdas P, Mayet J, Negus R, Patel N, Pierce I, Russell G, Wolff A, Xue H, Kellman P, Moon JC, Treibel TA, Cole GD, Fontana M. Patterns of myocardial injury in recovered troponin-positive COVID-19 patients assessed by cardiovascular magnetic resonance. Eur Heart J. 2021;42(19):1866–1878. - PMC - PubMed
-
- Tanacli R, Doeblin P, Götze C, Zieschang V, Faragli A, Stehning C, Korosoglou G, Erley J, Weiss J, Berger A, Pröpper F, Steinbeis F, Kühne T, Seidel F, Geisel D, Cannon Walter-Rittel T, Stawowy P, Witzenrath M, Klingel K, Van Linthout S, Pieske B, Tschöpe C, Kelle S. COVID-19 vs. classical myocarditis associated myocardial injury evaluated by cardiac magnetic resonance and endomyocardial biopsy. Front Cardiovasc Med. 2021;8:737257. - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous