

Fractional flow reserve measurements and long-term mortality-results from the FLORIDA study
- PMID: 38404721
- PMCID: PMC10885355
- DOI: 10.3389/fcvm.2024.1337941
Fractional flow reserve measurements and long-term mortality-results from the FLORIDA study
Abstract
Background: Randomized evidence suggested improved outcomes in fractional flow reserve (FFR) guidance of coronary revascularization compared to medical therapy in well-defined patient cohorts. However, the impact of FFR-guided revascularization on long-term outcomes of unselected patients with chronic or acute coronary syndromes (ACS) is unknown.
Aims: The FLORIDA (Fractional FLOw Reserve In cardiovascular DiseAses) study sought to investigate outcomes of FFR-guided vs. angiography-guided treatment strategies in a large, real-world cohort.
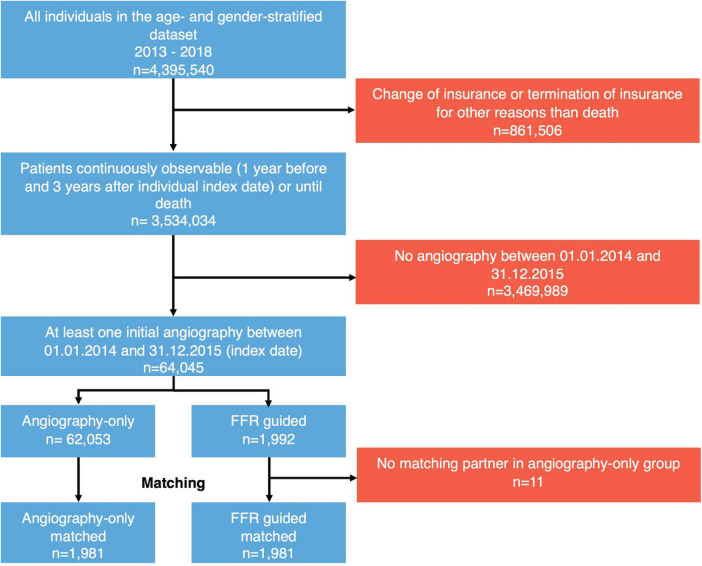
Methods: This study included patients enrolled into the German InGef Research Database. Patients undergoing coronary angiography between January 2014 and December 2015 were included in the analysis. Eligible patients had at least one inpatient coronary angiogram for suspected coronary artery disease between January 2014 and December 2015. Patients were stratified into FFR arm if a coronary angiography with adjunctive FFR measurement was performed, otherwise into the angiography-only arm. Matching was applied to ensure a balanced distribution of baseline characteristics in the study cohort. Patients were followed for 3 years after index date and primary endpoint was all-cause mortality.
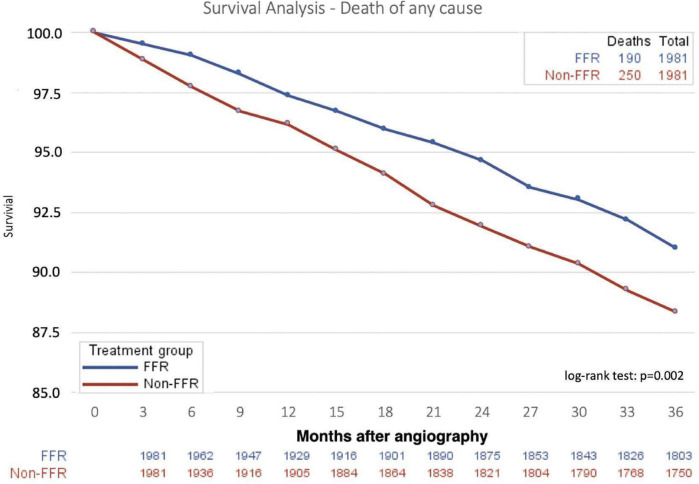
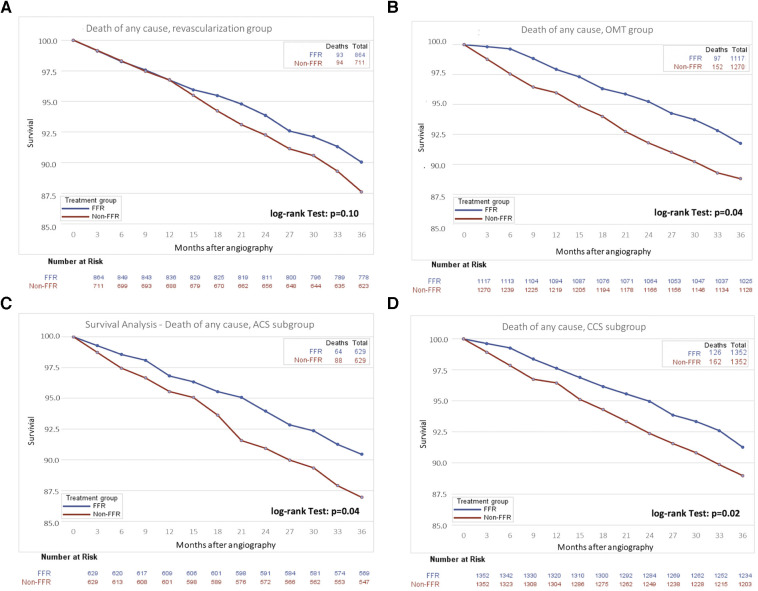
Results: In the matched population, mortality at 3 years was 9.6% in the FFR-assessed group and 12.6% in the angiography-only group (p = 0.002), corresponding to a 24% relative risk reduction with use of FFR. This effect was most pronounced in patients in whom revascularization was deferred based on FFR (8.7% vs. 12.3%, p = 0.04) and in high-risk subgroups including patients aged ≥75 years (14.9% vs. 20.1%, p < 0.01) and those presenting with ACS (10.2% vs. 14.0%, p = 0.04).
Conclusions: FFR-based revascularization strategy was associated with reduced mortality at 3 years. These findings further support the use of FFR in everyday clinical practice.
Keywords: acute coronary syndrome; chronic coronary syndrome; fractional flow reserve; mortality; percutaneous coronary intervention; real-world evidence.
© 2024 Boeckling, Stähli, Rudolph, Lutz, Schatz, Vogelmann, Stueve, West, Boone, Erbay and Leistner.
Conflict of interest statement
BS reports grants from Boston Scientific and grants from Edwards Lifesciences outside the submitted work. TR reports personal fees from Vulcano Philips and personal fees from Abbott Vascular outside the submitted work. ML reports grants, personal fees and other from Abbott Medical during the conduct of the study. TV reports grants from Abbott Vascular during the conduct of the study, personal fees from Abbott Vascular, personal fees from B. Braun, personal fees from In review Boston Scientific, personal fees from Edwards Lifescience, all outside the submitted work. MS, NW and EB are employees of Abbott Vascular. DL reports personal fees and non-financial support from Abbott Vascular, during the conduct of the study, personal fees from Boston Scientific, grants and personal fees from Abbott Vascular outside the submitted work. FB, AS-S, and AE have nothing to disclose. The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Figures
References
-
- Xiu J, Chen G, Zheng H, Wang Y, Chen H, Liu X, et al. Comparing treatment outcomes of fractional flow reserve-guided and angiography-guided percutaneous coronary intervention in patients with multi-vessel coronary artery diseases: a systematic review and meta-analysis. Clin Invest Med. (2016) 39(1):E25–36. 10.25011/cim.v39i1.26327 - DOI - PubMed
-
- Patel MR, Calhoon JH, Dehmer GJ, Grantham JA, Maddox TM, Maron DJ, et al. ACC/AATS/AHA/ASE/ASNC/SCAI/SCCT/STS 2017 appropriate use criteria for coronary revascularization in patients with stable ischemic heart disease: a report of the American college of cardiology appropriate use criteria task force, American association for thoracic surgery, American heart association, American society of echocardiography, American society of nuclear cardiology, society for cardiovascular angiography and interventions, society of cardiovascular computed tomography, and society of thoracic surgeons. J Am Coll Cardiol. (2017) 69(17):2212–41. 10.1016/j.jacc.2017.02.001 - DOI - PubMed
LinkOut - more resources
Full Text Sources