

Adherence to lung protective mechanical ventilation in patients admitted to a surgical intensive care unit and the associated increased mortality
- PMID: 38404779
- PMCID: PMC10884462
- DOI: 10.1016/j.heliyon.2024.e26220
Adherence to lung protective mechanical ventilation in patients admitted to a surgical intensive care unit and the associated increased mortality
Abstract
Background: The adherence rate to the lung protective ventilation (LPV) strategy, which is generally accepted as a standard practice in mechanically ventilated patients, reported in the literature is approximately 40%. This study aimed to determine the adherence rate to the LPV strategy, factors associated with this adherence, and related clinical outcomes in mechanically ventilated patients admitted to the surgical intensive care unit (SICU).
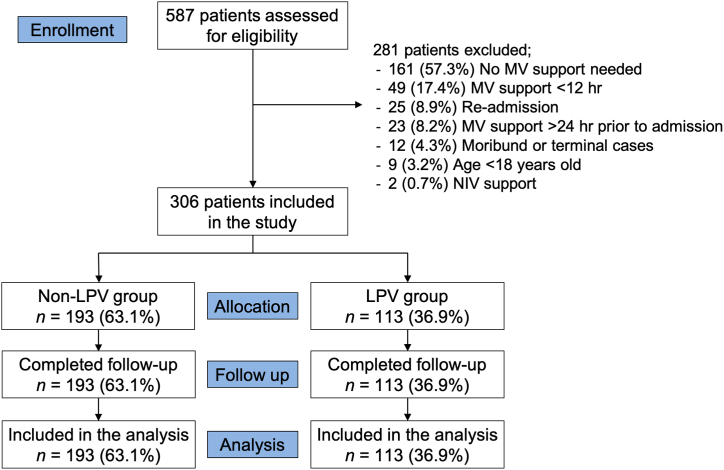
Methods: This prospective observational study was conducted in the SICU of a tertiary university-based hospital between April 2018 and February 2019. Three hundred and six adult patients admitted to the SICU who required mechanical ventilation support for more than 12 h were included. Ventilator parameters at the initiation of mechanical ventilation support in the SICU were recorded. The LPV strategy was defined as ventilation with a tidal volume of equal or less than 8 ml/kg of predicted body weight plus positive end-expiratory pressure of at least 5 cm H2O. Demographic and clinical data were recorded and analyzed.
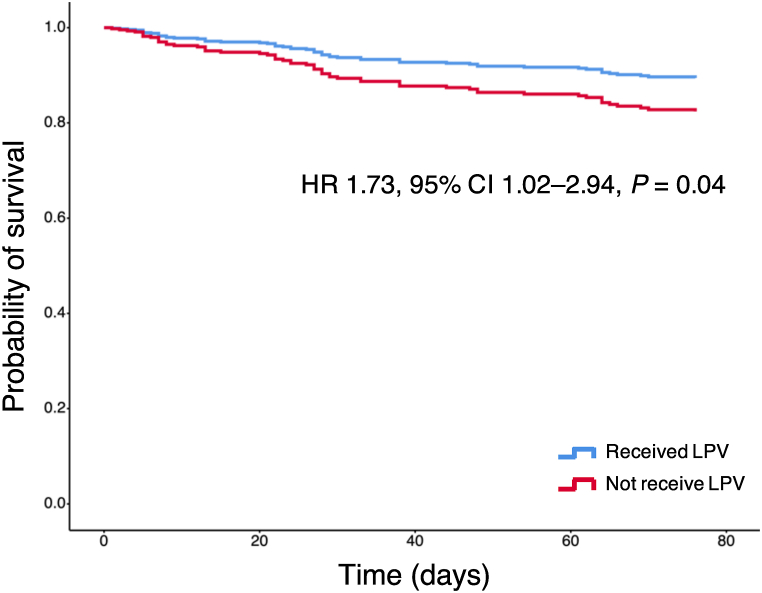
Results: There were 306 patients included in this study. The adherence rate to the LPV strategy was 36.9%. Height was the only factor associated with adherence to the LPV strategy (odds ratio for each cm, 1.10; 95% confidence interval (CI), 1.06-1.15). Cox regression analysis showed that the LPV strategy was associated with increased 90-day mortality (hazard ratio, 1.73; 95% CI, 1.02-2.94).
Conclusion: The adherence rate to the LPV strategy among patients admitted to the SICU was modest. Further studies are warranted to explore whether the application of the LPV strategy is simply a marker of disease severity or a causative factor for increased mortality.
Keywords: Adherence; Intensive care unit; Lung protective ventilation; Mortality; Surgical patients; Tidal volume.
© 2024 The Authors.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- Biehl M., Kashiouris M.G., Gajic O. Ventilator-induced lung injury: minimizing its impact in patients with or at risk for ARDS. Respir. Care. 2013;58(6):927–937. - PubMed
-
- Terragni P., Ranieri V.M., Brazzi L. Novel approaches to minimize ventilator-induced lung injury. Curr. Opin. Crit. Care. 2015;21(1):20–25. - PubMed
-
- Neto A.S., Cardoso S.O., Manetta J.A., et al. Association between use of lung-protective ventilation with lower tidal volumes and clinical outcomes among patients without acute respiratory distress syndrome: a meta-analysis. JAMA. 2012;308(16):1651–1659. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
