

Racial disparities in staging, treatment, and mortality in non-small cell lung cancer
- PMID: 38405005
- PMCID: PMC10891396
- DOI: 10.21037/tlcr-23-407
Racial disparities in staging, treatment, and mortality in non-small cell lung cancer
Abstract
Background: Black race is associated with advanced stage at diagnosis and increased mortality in non-small cell lung cancer (NSCLC). Most studies focus on race alone, without accounting for social determinants of health (SDOH). We explored the hypothesis that racial disparities in stage at diagnosis and outcomes are associated with SDOH and influence treatment decisions by patients and providers.
Methods: Patients with NSCLC newly diagnosed at Indiana University Simon Comprehensive Cancer Center (IUSCCC) from January 1, 2000 to May 31, 2015 were studied. Multivariable regression analyses were conducted to examine the impact of SDOH (race, gender, insurance status, and marital status) on diagnosis stage, time to treatment, receipt of and reasons for not receiving guideline concordant treatment, and 5-year overall survival (OS) based on Kaplan-Meier curves.
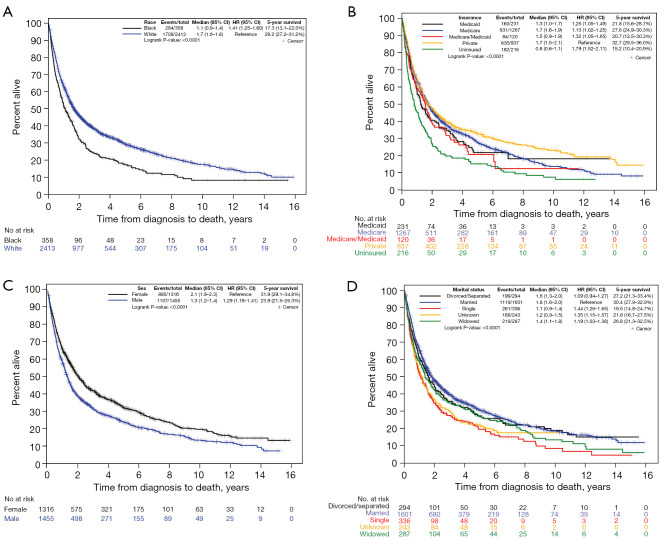
Results: A total of 3,349 subjects were included in the study, 12.2% of Black race. Those diagnosed with advanced-stage NSCLC had a significantly higher odds of being male, uninsured, and Black. Five-year OS was lower in those of Black race, male, single, uninsured, Medicare/Medicaid insurance, and advanced stage. Adjusted for multiple variables, individuals with Medicare, Medicare/Medicaid, uninsured, widowed, and advanced stage at diagnosis, were associated with significantly lower OS time. Black, single, widowed, and uninsured individuals were less likely to receive stage appropriate treatment for advanced disease. Those uninsured [odds ratio (OR): 3.876, P<0.001], Medicaid insurance (OR: 3.039, P=0.0017), and of Black race (OR: 1.779, P=0.0377) were less likely to receive curative-intent surgery for early-stage NSCLC because it was not a recommended treatment.
Conclusions: We found racial, gender, and socioeconomic disparities in NSCLC diagnosis stage, receipt of stage-appropriate treatment, and reasons for guideline discordance in receipt of curative intent surgery for early-stage NSCLC. While insurance type and marital status were associated with worse OS, race alone was not. This suggests racial differences in outcomes may not be associated with race alone, but rather worse SDOH disproportionately affecting Black individuals. Efforts to understand advanced diagnosis and reasons for failure to receive stage-appropriate treatment by vulnerable populations is needed to ensure equitable NSCLC care.
Keywords: Race; insurance; lung cancer; socioeconomic; surgery.
2024 Translational Lung Cancer Research. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://tlcr.amegroups.com/article/view/10.21037/tlcr-23-407/coif). F.C.D. reports this research was funded in part by training grants from the NIH-NRSA (No. TL1 TR002531) and NIH-NHLBI (No. 5R25-HL126140-08 PRIDE-AiRE). N.A.N. reports funding to Indiana University School of Medicine in the form of a training grant (NIH-NHLBI, No. T32HL091816). L.N. has a research grant from Delfi Diagnostics. They paid the grant directly to his institution. C.R.S. reports this research was funded in part by the American Cancer Society (Grant No. 128511-MRSG-15-163-01-DMC) and the U.S. Department of Veterans Affairs BLR&D, Merit Review (Grant No. I01-BX005353). She provides unpaid service related to lung cancer screening for National Comprehensive Cancer Network (NCCN, Lung Cancer Screening Guidelines panel) that is not directly related to the research performed in this manuscript. The other authors have no conflicts of interest to declare.
Figures
Similar articles
-
Racial/ethnic disparities in curative-intent treatment for early-stage non-small cell lung cancer patients among heterogeneous Black populations: US-born Black, Afro-Haitian, West Indian Black, and Hispanic Black.Cancer Med. 2024 Oct;13(19):e7449. doi: 10.1002/cam4.7449. Cancer Med. 2024. PMID: 39377643 Free PMC article.
-
Variations in Receipt of Curative-Intent Surgery for Early-Stage Non-Small Cell Lung Cancer (NSCLC) by State.J Thorac Oncol. 2016 Jun;11(6):880-9. doi: 10.1016/j.jtho.2016.03.003. Epub 2016 Mar 12. J Thorac Oncol. 2016. PMID: 26980472
-
Influence of Race, Insurance, and Rurality on Equity of Breast Cancer Care.J Surg Res. 2022 Mar;271:117-124. doi: 10.1016/j.jss.2021.09.042. Epub 2021 Dec 8. J Surg Res. 2022. PMID: 34894544
-
Disparities in the surgical management of early stage non-small cell lung cancer: how far have we come?J Thorac Dis. 2019 Mar;11(Suppl 4):S596-S611. doi: 10.21037/jtd.2019.01.63. J Thorac Dis. 2019. PMID: 31032078 Free PMC article. Review.
-
Sociodemographic disparities in the management of advanced lung cancer: a narrative review.J Thorac Dis. 2021 Jun;13(6):3772-3800. doi: 10.21037/jtd-20-3450. J Thorac Dis. 2021. PMID: 34277069 Free PMC article. Review.
Cited by
-
Systematic scoping review of external validation studies of AI pathology models for lung cancer diagnosis.NPJ Precis Oncol. 2025 Jun 7;9(1):166. doi: 10.1038/s41698-025-00940-7. NPJ Precis Oncol. 2025. PMID: 40483288 Free PMC article.
-
Repression of ZNFX1 by LncRNA ZFAS1 mediates tobacco-induced pulmonary carcinogenesis.Cell Mol Biol Lett. 2025 Apr 10;30(1):44. doi: 10.1186/s11658-025-00705-x. Cell Mol Biol Lett. 2025. PMID: 40211119 Free PMC article.
-
Racial disparities in non-small cell lung cancer survival outcomes: a systematic review and meta-analysis.Proc (Bayl Univ Med Cent). 2025 Jul 14;38(5):722-731. doi: 10.1080/08998280.2025.2524792. eCollection 2025. Proc (Bayl Univ Med Cent). 2025. PMID: 40821488 Free PMC article.
-
Trends in influenza- and pneumonia-related mortality in lung cancer patients from 1999 to 2022: a retrospective CDC WONDER analysis.Respir Res. 2025 Sep 1;26(1):267. doi: 10.1186/s12931-025-03336-0. Respir Res. 2025. PMID: 40890819 Free PMC article.
-
Dismal adherence to lung cancer screening in a diverse urban population.J Thorac Cardiovasc Surg. 2025 Jul;170(1):46-51.e1. doi: 10.1016/j.jtcvs.2024.12.007. Epub 2024 Dec 13. J Thorac Cardiovasc Surg. 2025. PMID: 39675415
References
Grants and funding
LinkOut - more resources
Full Text Sources
Medical