

Management of pasireotide-induced hyperglycemia in patients with acromegaly: An experts' consensus statement
- PMID: 38405148
- PMCID: PMC10884330
- DOI: 10.3389/fendo.2024.1348990
Management of pasireotide-induced hyperglycemia in patients with acromegaly: An experts' consensus statement
Abstract
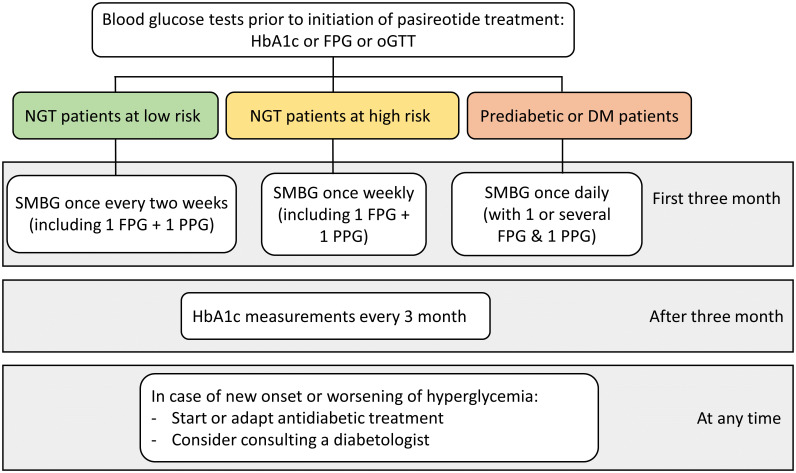
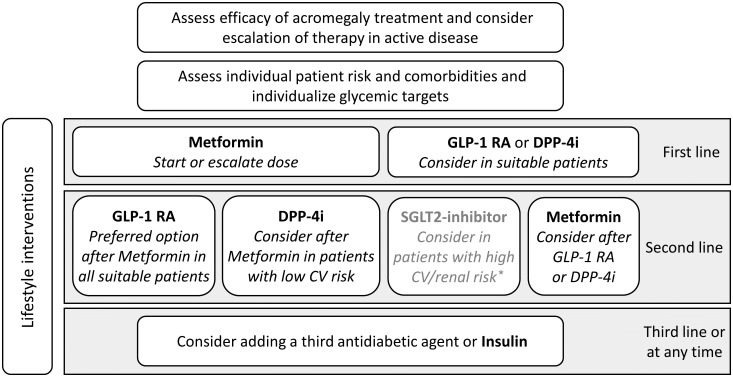
Pasireotide is a somatostatin analogue for the treatment of acromegaly, a chronic condition caused by excess growth hormone. Despite the therapeutic benefits of pasireotide as a second-line treatment for inadequately controlled acromegaly, a major concern is its hyperglycemic side-effect. Here, we provide guidance on how to select appropriate patients with acromegaly for treatment with pasireotide. We summarize baseline characteristics of patients at high risk for pasireotide-associated hyperglycemia and recommend a monitoring strategy based on the risk profile. Self-monitoring of blood glucose levels (SMBG), measurements of fasting plasma glucose (FPG), postprandial plasma glucose (PPG) and regular HbA1c measurements are the foundation of our proposed monitoring approach. The pathophysiology of pasireotide-induced hyperglycemia involves decreased secretion of the incretin hormones GIP (glucose-dependent insulinotropic polypeptide) and GLP-1 (glucagon-like peptide-1). Our expert recommendations address the specific pathophysiology of pasireotide-induced hyperglycemia by recommending the incretin-based therapeutics dipeptidyl peptidase-4 inhibitors (DPP-4i) and glucagon-like peptide-1 receptor agonists (GLP-1 RA) in all appropriate patients as an alternative to first-line monotherapy with metformin. Furthermore, we emphasize the importance of adequate control of acromegaly, excellent diabetes education, nutrition and lifestyle guidance and advise to consult expert diabetologists in case of uncertainty in the management of patients with hyperglycemia under pasireotide.
Keywords: acromegaly; diabetes mellitus; hyperglycemia; monitoring strategy; pasireotide; patient management.
Copyright © 2024 Störmann, Meyhöfer, Groener, Faust, Schilbach, Seufert and Vergès.
Conflict of interest statement
SS has received consulting fees from Crinetics and Recordati Rare Diseases RRD as well as honoraria for lectures and conference chairing from Novartis, Ipsen, Hexal/Sandoz, Pfizer, and RRD. He has served as advisory board member for Novartis and RRD. Furthermore, RRD has donated a drug for compassionate use in one of his patients. SM has received lecturing fees and/or consulting fees and/or grants from AstraZeneca, Bayer, Boehringer Ingelheim, Lilly, Novo Nordisk, RRD. JG and JF have received consulting fees from RRD. KS has received lecturing fees and/or consulting fees from Pfizer, RRD, Sandoz, and Novo Nordisk. JS has received honoraria for talks and/or consultancy and/or research funding from Apitope, AstraZeneca, Bayer, Berlin Chemie, Boehringer Ingelheim, Bristol-Meyers Squibb, Eli Lilly, GI-Dynamics, GlaxoSmithKline, Intarcia, Ipsen, Janssen, LifeScan, MedScape, MSD, Novartis, Novo Nordisk, Omniamed, Pfizer, RRD, Roche, Sanofi, Servier, Takeda, and Ypsomed. In the past 3 years BV has received honoraria from Amgen, AstraZeneca, Lilly, Novo Nordisk, Sanofi and RRD for conferences or advisory boards, and received funding for research from AstraZeneca and Novo Nordisk.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical