

Minimally Invasive Open Cystogastrostomy for Giant Pancreatic Pseudocyst in Pediatric Patients
- PMID: 38405246
- PMCID: PMC10883164
- DOI: 10.4103/jiaps.jiaps_178_23
Minimally Invasive Open Cystogastrostomy for Giant Pancreatic Pseudocyst in Pediatric Patients
Abstract
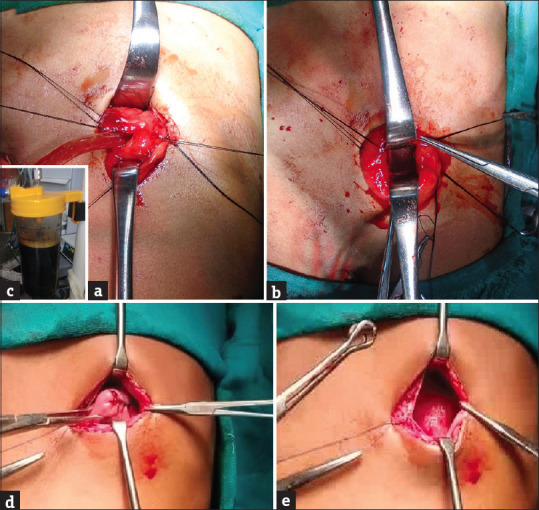
Open cystogastrostomy is the standard treatment for the operative management of pancreatic pseudocysts. We describe our technique of minimally invasive open cystogastrostomy for giant pediatric pancreatic pseudocyst. Preoperative incision marking on the most prominent part of the pseudocyst was done by ultrasound guidance. A transverse incision of approximately 3-4 cm was made, and a minilaparotomy was performed. Stay sutures were applied on the anterior wall of the stomach. The anterior wall was exteriorized; transverse gastrotomy was performed, and superior and inferior flaps were made. Deaver's retractor was placed inside the lumen, and cystogastrostomy was completed. We employed this technique in five male patients without any complications. All patients were allowed clear liquids on postoperative day 4 or 5; and gradually shifted to a soft diet. The mean duration of postoperative stay was 7 days. The size of the scar ranged from 3 to 5 cm. All patients were doing well on follow-up. Our technique of minimally invasive open cystogastrostomy is a viable option for pancreatic pseudocyst in pediatric patients.
Keywords: Cystogastrostomy; minimally invasive; open; pancreatic; pediatric; pseudocyst; trauma.
Copyright: © 2024 Journal of Indian Association of Pediatric Surgeons.
Conflict of interest statement
There are no conflicts of interest.
Figures

Similar articles
-
Laparoscopy-assisted open cystogastrostomy and pancreatic debridement for necrotizing pancreatitis (with video).Surg Endosc. 2016 Mar;30(3):1235-41. doi: 10.1007/s00464-015-4331-6. Epub 2015 Aug 15. Surg Endosc. 2016. PMID: 26275532
-
Laparoscopic cystogastrostomy for the treatment of pancreatic pseudocysts in children.J Pediatr Surg. 2005 Nov;40(11):e13-7. doi: 10.1016/j.jpedsurg.2005.07.041. J Pediatr Surg. 2005. PMID: 16291133
-
Intragastric cystogastrostomy in a 4-year-old child with a pancreatic pseudocyst: A novel technique.Afr J Paediatr Surg. 2018 Jul-Dec;15(3):148-150. doi: 10.4103/ajps.AJPS_71_17. Afr J Paediatr Surg. 2018. PMID: 32769368 Free PMC article.
-
[Endoscopic ultrasound-guided cystogastrostomy for successful drainage of pancreatic pseudocyst: a pediatric case report].Nihon Shokakibyo Gakkai Zasshi. 2016;113(1):71-7. doi: 10.11405/nisshoshi.113.71. Nihon Shokakibyo Gakkai Zasshi. 2016. PMID: 26743556 Review. Japanese.
-
Laparoscopic pancreatic cystgastrostomy.J Hepatobiliary Pancreat Surg. 2000;7(1):28-34. doi: 10.1007/s005340050150. J Hepatobiliary Pancreat Surg. 2000. PMID: 10982588 Review.
Cited by
-
Transmesocolic Cystojejunoanastomosis in a Mexican Patient With a Giant Post-acute Pancreatic Pseudocyst Following Acute Pancreatitis: A Case Report.Cureus. 2025 Aug 1;17(8):e89228. doi: 10.7759/cureus.89228. eCollection 2025 Aug. Cureus. 2025. PMID: 40761371 Free PMC article.
References
-
- Hassan MA. Open cystogastrostomy in the management of a large pancreatic pseudocyst in a child. J Pediatr Surg Case Rep. 2020;59:1–3.
-
- Makris KI, St Peter SD, Tsao KJ, Ostlie DJ. Laparoscopic intragastric stapled cystgastrostomy of pancreatic pseudocyst in a child. J Laparoendosc Adv Surg Tech A. 2008;18:771–3. - PubMed
LinkOut - more resources
Full Text Sources