

Role of Cerebroplacental Ratio in Predicting Perinatal Outcome
- PMID: 38405647
- PMCID: PMC10893822
- DOI: 10.7759/cureus.54816
Role of Cerebroplacental Ratio in Predicting Perinatal Outcome
Abstract
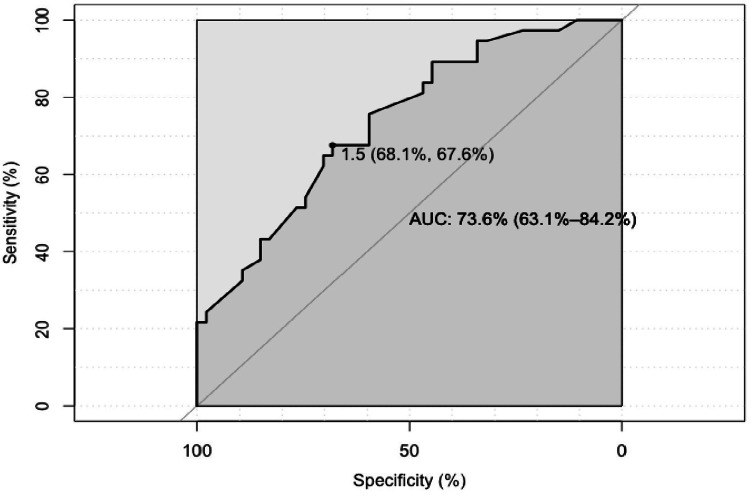
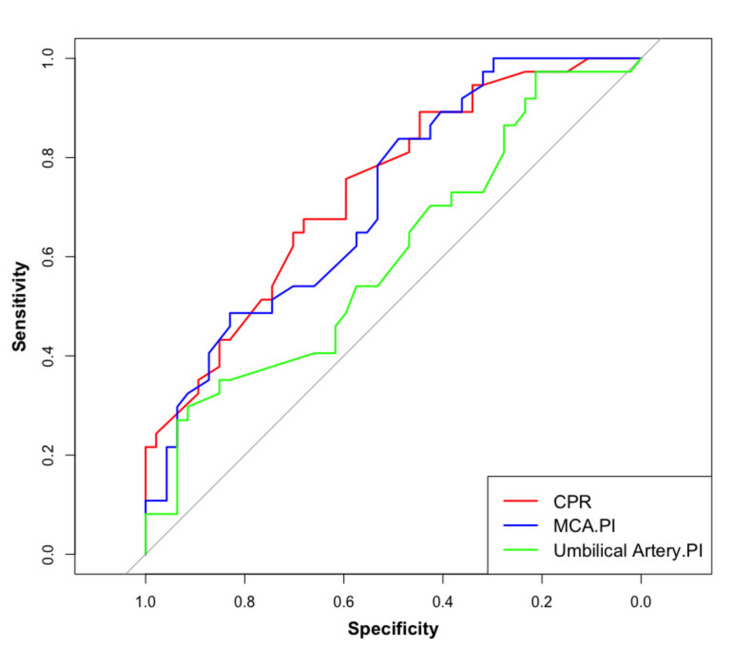
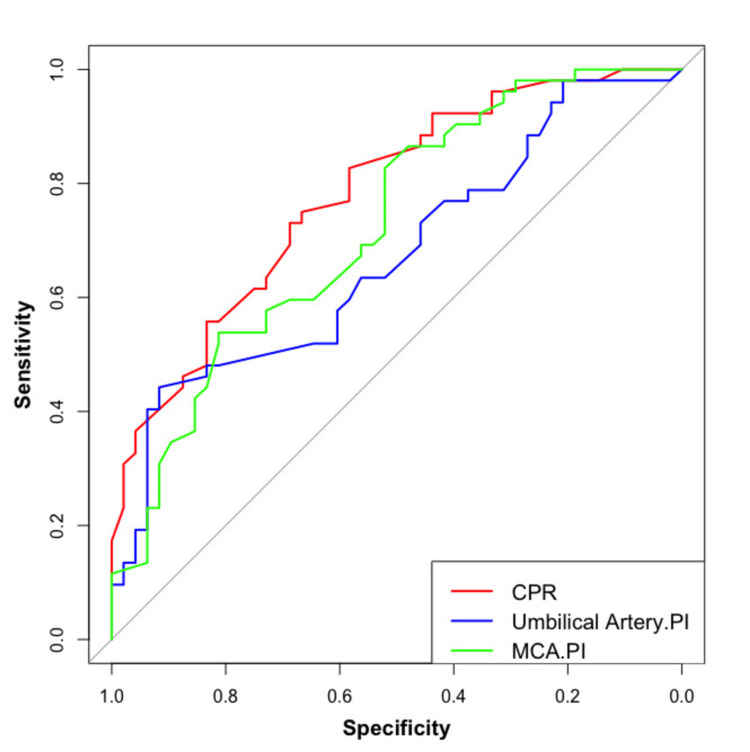
Objective Doppler velocimetry provides a sensitive, non-invasive, and safe method of surveillance of fetal hemodynamics and fetomaternal circulation. Cerebroplacental ratio (CPR) is an indicator of placental function and fetal maladaptation to placental insufficiency. Cerebroplacental ratio (CPR) is becoming a significant indicator of unfavorable pregnancy outcomes, which has implications for the assessment of fetal well-being. This study aimed to determine the cut-off value of the cerebroplacental ratio (CPR) in appropriate for gestational age (AGA) fetuses in high-risk mothers to predict adverse perinatal outcomes. We also compared the efficacy of CPR, umbilical artery pulsatility index (UmA PI), and middle cerebral artery pulsatility index (MCA PI) for predicting adverse perinatal outcomes. Design and setting This was a prospective observational study conducted at the Postgraduate Institute of Medical Education and Research (PGIMER), Chandigarh, India. Methods A total of 100 women with singleton high-risk pregnancies were included in this prospective observational study. Obstetric ultrasound was performed at the time of recruitment, and fetal weight and CPR were noted. Based on fetal weight, patients were divided into AGA and fetal growth restriction (FGR) groups; CPR was measured; patients were followed up fortnightly; and outcomes were noted. Main outcome The effectiveness of CPR, UmA PI, and MCA PI for predicting poor perinatal outcomes and identifying the cut-off value of CPR in appropriate for gestational age (AGA) fetuses in high-risk mothers was assessed. Result The values of MCA PI, UmA PI, and CPR were statistically significant between AGA and FGR (p-value =.023, .002 and .0001), respectively. The cut-off value for CPR-detecting adverse outcomes in AGA was 1.49. It has sensitivity, specificity, positive predictive value, and negative predictive value of 67.5%, 68%, 71.69%, and 70.21%, respectively. Conclusion Cerebroplacental ratio (CPR) reflects both circulatory insufficiency of the placenta and adaptive changes of the middle cerebral artery, indicating an important non-invasive surveillance modality.
Keywords: cerebroplacental ratio; high-risk pregnancy; middle cerebral artery doppler; perinatal outcome; umbilical artery doppler.
Copyright © 2024, Kumar et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Role of Doppler ultrasound at time of diagnosis of late-onset fetal growth restriction in predicting adverse perinatal outcome: prospective cohort study.Ultrasound Obstet Gynecol. 2020 Jun;55(6):793-798. doi: 10.1002/uog.20406. Epub 2020 May 8. Ultrasound Obstet Gynecol. 2020. PMID: 31343783
-
Routine assessment of cerebroplacental ratio at 35-37 weeks' gestation in the prediction of adverse perinatal outcome.Am J Obstet Gynecol. 2019 Jul;221(1):65.e1-65.e18. doi: 10.1016/j.ajog.2019.03.002. Epub 2019 Mar 13. Am J Obstet Gynecol. 2019. PMID: 30878322
-
Cerebroplacental ratio as predictor of adverse perinatal outcome in the third trimester.Acta Obstet Gynecol Scand. 2021 Mar;100(3):497-503. doi: 10.1111/aogs.14031. Epub 2020 Nov 4. Acta Obstet Gynecol Scand. 2021. PMID: 33078387 Free PMC article.
-
Comparison between cerebroplacental ratio and umbilicocerebral ratio in predicting adverse perinatal outcome at term.Eur J Obstet Gynecol Reprod Biol. 2020 Sep;252:439-443. doi: 10.1016/j.ejogrb.2020.07.032. Epub 2020 Jul 24. Eur J Obstet Gynecol Reprod Biol. 2020. PMID: 32763648 Review.
-
Predictive accuracy of cerebroplacental ratio for adverse perinatal and neurodevelopmental outcomes in suspected fetal growth restriction: systematic review and meta-analysis.Ultrasound Obstet Gynecol. 2018 Oct;52(4):430-441. doi: 10.1002/uog.19117. Epub 2018 Sep 5. Ultrasound Obstet Gynecol. 2018. PMID: 29920817
References
-
- The NICHD neonatal research network: changes in practice and outcomes during the first 15 years. Fanaroff AA, Hack M, Walsh MC. Seminars in perinatology. 2003;27:281–287. - PubMed
-
- Anderson MS, Hay WW. Philadelphia: Lippincott Williams and Wilkins; 1999. Intrauterine Growth Restriction and the Small-for-Gestational Age Infant.
-
- Levels and patterns of intrauterine growth retardation in developing countries. de Onis M, Blössner M, Villar J. https://pubmed.ncbi.nlm.nih.gov/9511014/ Eur J Clin Nutr. 1998;52 Suppl 1:0–15. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous