

This is a preprint.
Machine Learning Predicts Cerebral Vasospasm in Subarachnoid Hemorrhage Patients
- PMID: 38405758
- PMCID: PMC10889065
- DOI: 10.21203/rs.3.rs-3617246/v1
Machine Learning Predicts Cerebral Vasospasm in Subarachnoid Hemorrhage Patients
Update in
-
Machine learning predicts cerebral vasospasm in patients with subarachnoid haemorrhage.EBioMedicine. 2024 Jul;105:105206. doi: 10.1016/j.ebiom.2024.105206. Epub 2024 Jun 19. EBioMedicine. 2024. PMID: 38901147 Free PMC article.
Abstract
Background: Cerebral vasospasm (CV) is a feared complication occurring in 20-40% of patients following subarachnoid hemorrhage (SAH) and is known to contribute to delayed cerebral ischemia. It is standard practice to admit SAH patients to intensive care for an extended period of vigilant, resource-intensive, clinical monitoring. We used machine learning to predict CV requiring verapamil (CVRV) in the largest and only multi-center study to date.
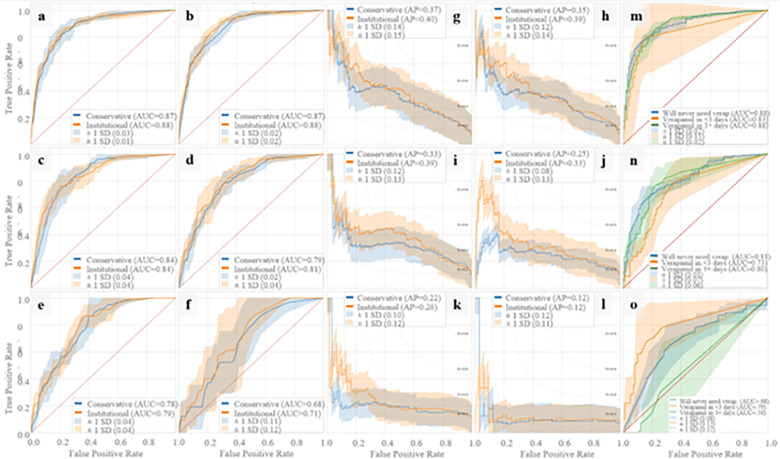
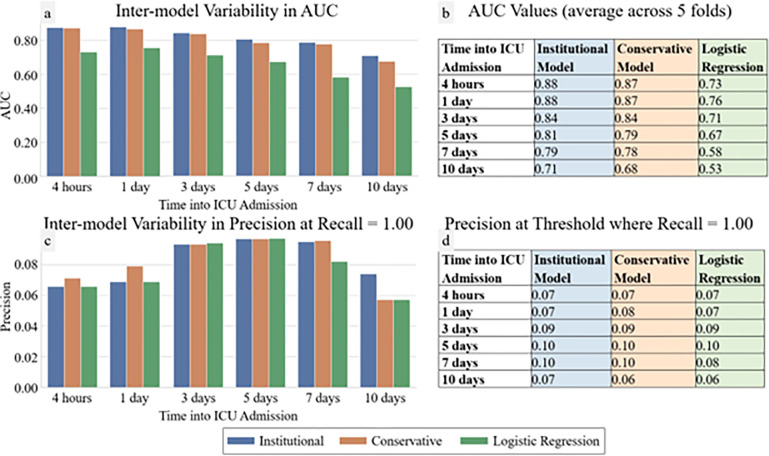
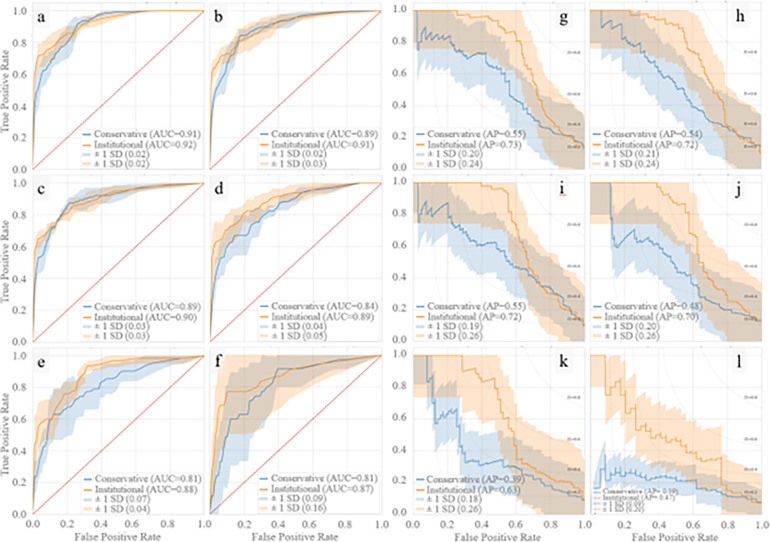
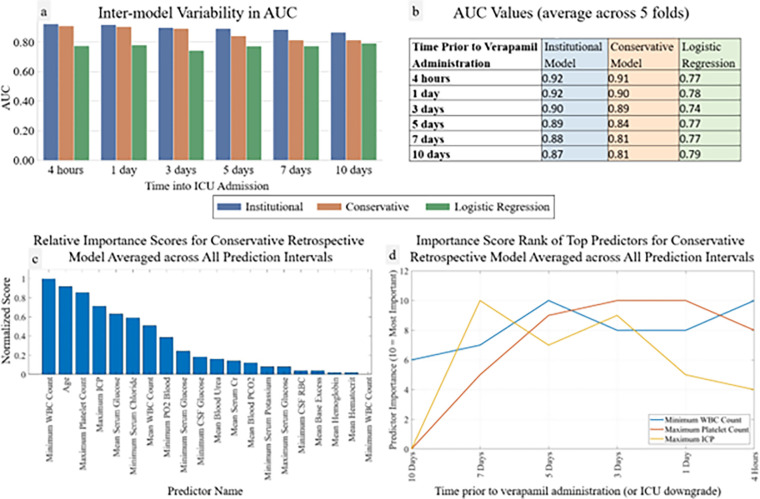
Methods: SAH patients admitted to UCLA from 2013-2022 and a validation cohort from VUMC from 2018-2023 were included. For each patient, 172 unique intensive care unit (ICU) variables were extracted through the primary endpoint, namely first verapamil administration or ICU downgrade. At each institution, a light gradient boosting machine (LightGBM) was trained using five- fold cross validation to predict the primary endpoint at various timepoints during hospital admission. Receiver-operator curves (ROC) and precision-recall (PR) curves were generated.
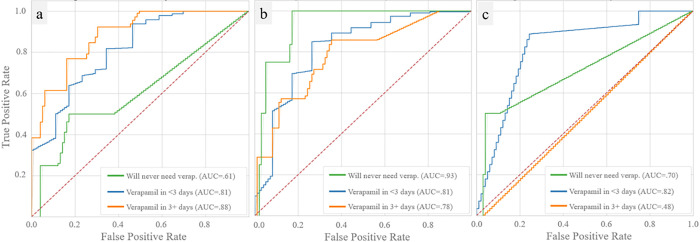
Results: A total of 1,750 patients were included from UCLA, 125 receiving verapamil. LightGBM achieved an area under the ROC (AUC) of 0.88 an average of over one week in advance, and successfully ruled out 8% of non-verapamil patients with zero false negatives. Minimum leukocyte count, maximum platelet count, and maximum intracranial pressure were the variables with highest predictive accuracy. Our models predicted "no CVRV" vs "CVRV within three days" vs "CVRV after three days" with AUCs=0.88, 0.83, and 0.88, respectively. For external validation at VUMC, 1,654 patients were included, 75 receiving verapamil. Predictive models at VUMC performed very similarly to those at UCLA, averaging 0.01 AUC points lower.
Conclusions: We present an accurate (AUC=0.88) and early (>1 week prior) predictor of CVRV using machine learning over two large cohorts of subarachnoid hemorrhage patients at separate institutions. This represents a significant step towards optimized clinical management and improved resource allocation in the intensive care setting of subarachnoid hemorrhage patients.
Conflict of interest statement
Disclosures The authors have no conflicts of interest or disclosures.
Figures
References
-
- Dorsch N. W. C. & King M. T. A review of cerebral vasospasm in aneurysmal subarachnoid haemorrhage Part I: Incidence and effects. J Clin Neurosci 1, 19–26 (1994). - PubMed
-
- EEG Monitoring to Detect Vasospasm after Subarachnoid Hemorrhage |…https://www.reliasmedia.com/articles/34004-eeg-monitoring-to-detect-vaso....
-
- Frontera J. A. et al. Defining Vasospasm After Subarachnoid Hemorrhage. Stroke 40, 1963–1968 (2009). - PubMed
-
- Diringer M. N. et al. Critical care management of patients following aneurysmal subarachnoid hemorrhage: recommendations from the Neurocritical Care Society’s Multidisciplinary Consensus Conference. Neurocrit Care 15, 211–240 (2011). - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
