

This is a preprint.
Adiposity and cancer: meta-analysis, mechanisms, and future perspectives
- PMID: 38405761
- PMCID: PMC10889047
- DOI: 10.1101/2024.02.16.24302944
Adiposity and cancer: meta-analysis, mechanisms, and future perspectives
Abstract
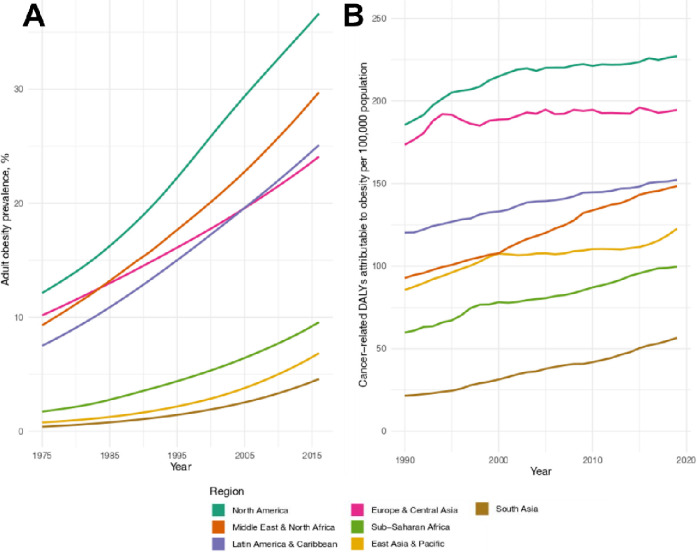
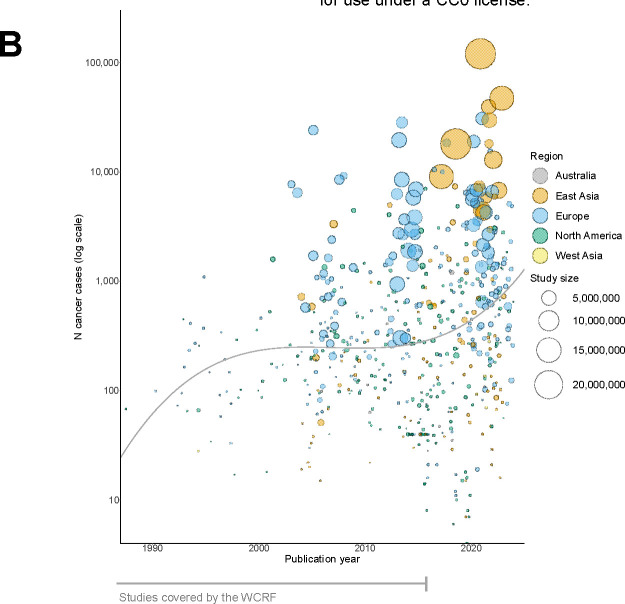
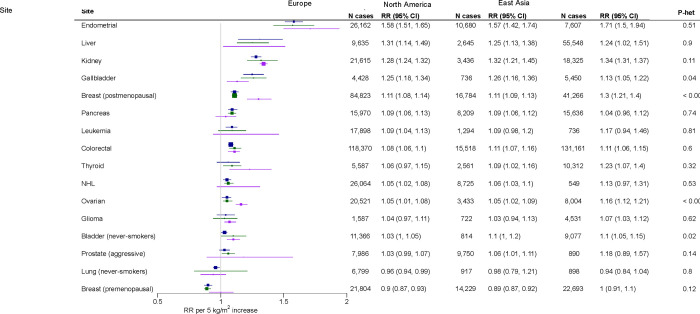
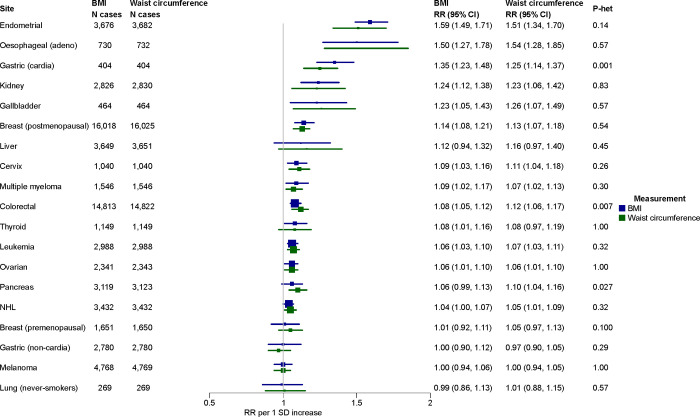
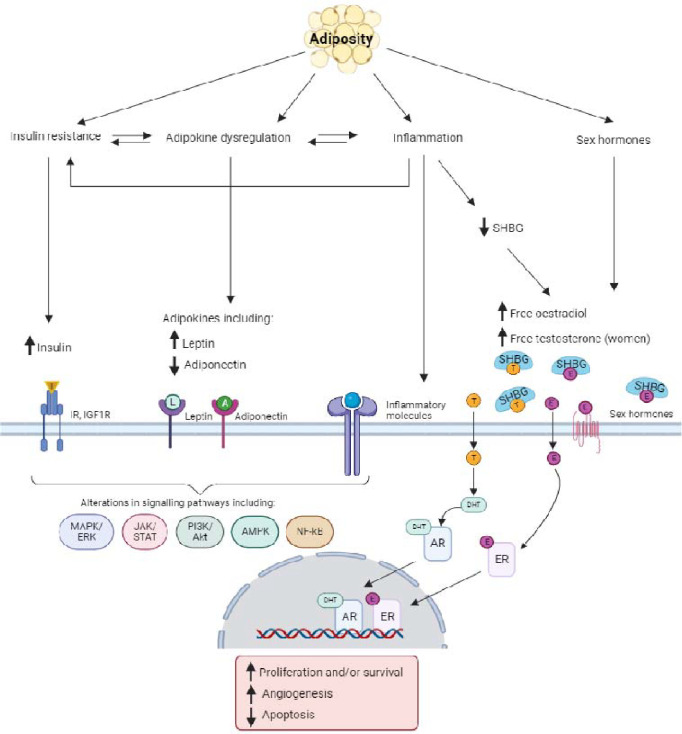
Obesity is a recognised risk factor for many cancers and with rising global prevalence, has become a leading cause of cancer. Here we summarise the current evidence from both population-based epidemiologic investigations and experimental studies on the role of obesity in cancer development. This review presents a new meta-analysis using data from 40 million individuals and reports positive associations with 19 cancer types. Utilising major new data from East Asia, the meta-analysis also shows that the strength of obesity and cancer associations varies regionally, with stronger relative risks for several cancers in East Asia. This review also presents current evidence on the mechanisms linking obesity and cancer and identifies promising future research directions. These include the use of new imaging data to circumvent the methodological issues involved with body mass index and the use of omics technologies to resolve biologic mechanisms with greater precision and clarity.
Conflict of interest statement
Ethics declarations Competing interests The authors declare no competing interests.
Figures



Similar articles
-
The Obesity Paradox in Cancer: Epidemiologic Insights and Perspectives.Curr Nutr Rep. 2019 Sep;8(3):175-181. doi: 10.1007/s13668-019-00280-6. Curr Nutr Rep. 2019. PMID: 31129887 Review.
-
The future of Cochrane Neonatal.Early Hum Dev. 2020 Nov;150:105191. doi: 10.1016/j.earlhumdev.2020.105191. Epub 2020 Sep 12. Early Hum Dev. 2020. PMID: 33036834
-
Understanding the Co-Epidemic of Obesity and COVID-19: Current Evidence, Comparison with Previous Epidemics, Mechanisms, and Preventive and Therapeutic Perspectives.Curr Obes Rep. 2021 Sep;10(3):214-243. doi: 10.1007/s13679-021-00436-y. Epub 2021 Apr 28. Curr Obes Rep. 2021. PMID: 33909265 Free PMC article. Review.
-
Body fatness associations with cancer: evidence from recent epidemiological studies and future directions.Metabolism. 2022 Dec;137:155326. doi: 10.1016/j.metabol.2022.155326. Epub 2022 Oct 1. Metabolism. 2022. PMID: 36191637 Review.
-
Anthropometric and adiposity indicators and risk of type 2 diabetes: systematic review and dose-response meta-analysis of cohort studies.BMJ. 2022 Jan 18;376:e067516. doi: 10.1136/bmj-2021-067516. BMJ. 2022. PMID: 35042741 Free PMC article.
References
-
- Blitzer P. H., Blitzer E. C. & Rimm A. A. Association between teen-age obesity and cancer in 56,111 women: all cancers and endometrial carcinoma. Prev. Med. 5, 20–31 (1976). - PubMed
-
- de Waard F. & Baanders-van Halewijn E. A. A prospective study in general practice on breast-cancer risk in postmenopausal women. Int. J. Cancer 14, 153–160 (1974). - PubMed
-
- Wynder E. L., Escher G. C. & Mantel N. An epidemiological investigation of cancer of the endometrium. Cancer 19, 489–520 (1966). - PubMed
-
- AICR. The AICR 2015 Cancer Risk Awareness Survey Report. (2015).
Publication types
LinkOut - more resources
Full Text Sources