

This is a preprint.
Alterations in Lysosomal, Glial and Neurodegenerative Biomarkers in Patients with Sporadic and Genetic Forms of Frontotemporal Dementia
- PMID: 38405775
- PMCID: PMC10888909
- DOI: 10.1101/2024.02.09.579529
Alterations in Lysosomal, Glial and Neurodegenerative Biomarkers in Patients with Sporadic and Genetic Forms of Frontotemporal Dementia
Abstract
Background: Frontotemporal dementia (FTD) is the most common cause of early-onset dementia with 10-20% of cases caused by mutations in one of three genes: GRN, C9orf72, or MAPT. To effectively develop therapeutics for FTD, the identification and characterization of biomarkers to understand disease pathogenesis and evaluate the impact of specific therapeutic strategies on the target biology as well as the underlying disease pathology are essential. Moreover, tracking the longitudinal changes of these biomarkers throughout disease progression is crucial to discern their correlation with clinical manifestations for potential prognostic usage.
Methods: We conducted a comprehensive investigation of biomarkers indicative of lysosomal biology, glial cell activation, synaptic and neuronal health in cerebrospinal fluid (CSF) and plasma from non-carrier controls, sporadic FTD (symptomatic non-carriers) and symptomatic carriers of mutations in GRN, C9orf72, or MAPT, as well as asymptomatic GRN mutation carriers. We also assessed the longitudinal changes of biomarkers in GRN mutation carriers. Furthermore, we examined biomarker levels in disease impacted brain regions including middle temporal gyrus (MTG) and superior frontal gyrus (SFG) and disease-unaffected inferior occipital gyrus (IOG) from sporadic FTD and symptomatic GRN carriers.
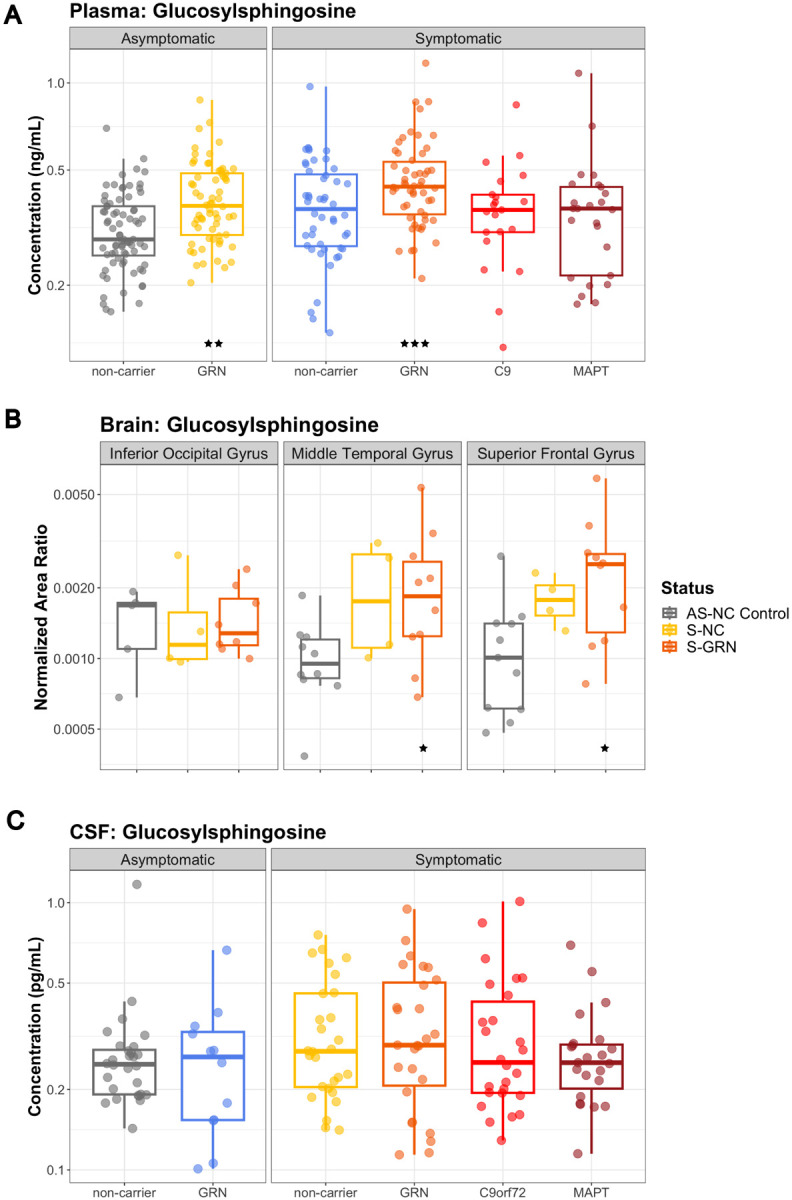
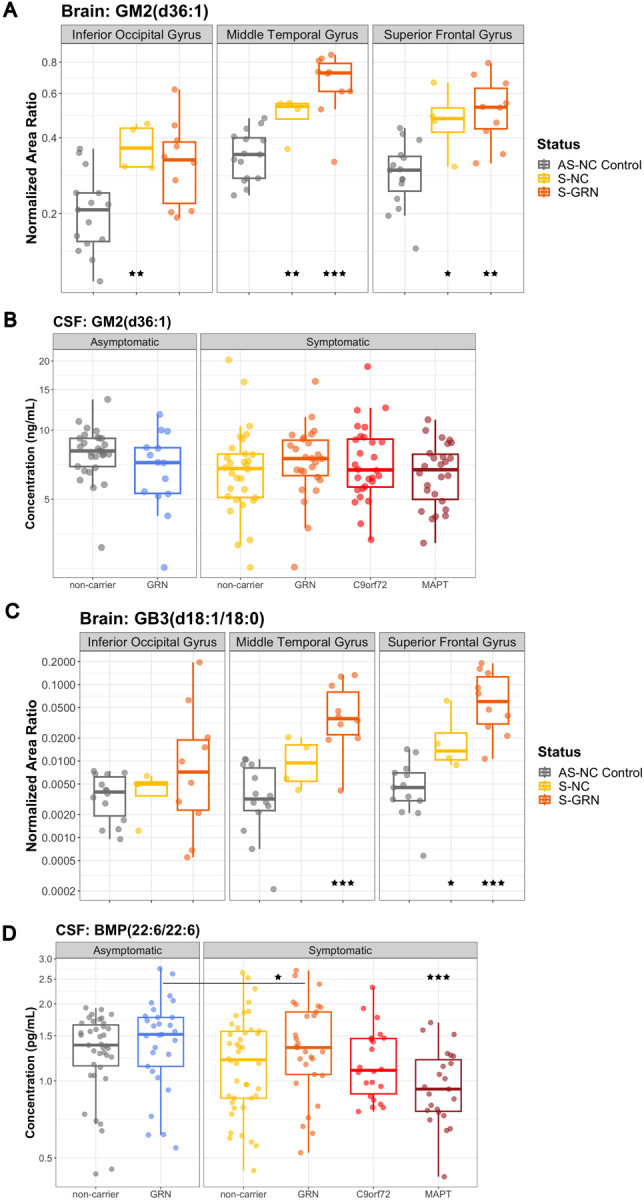
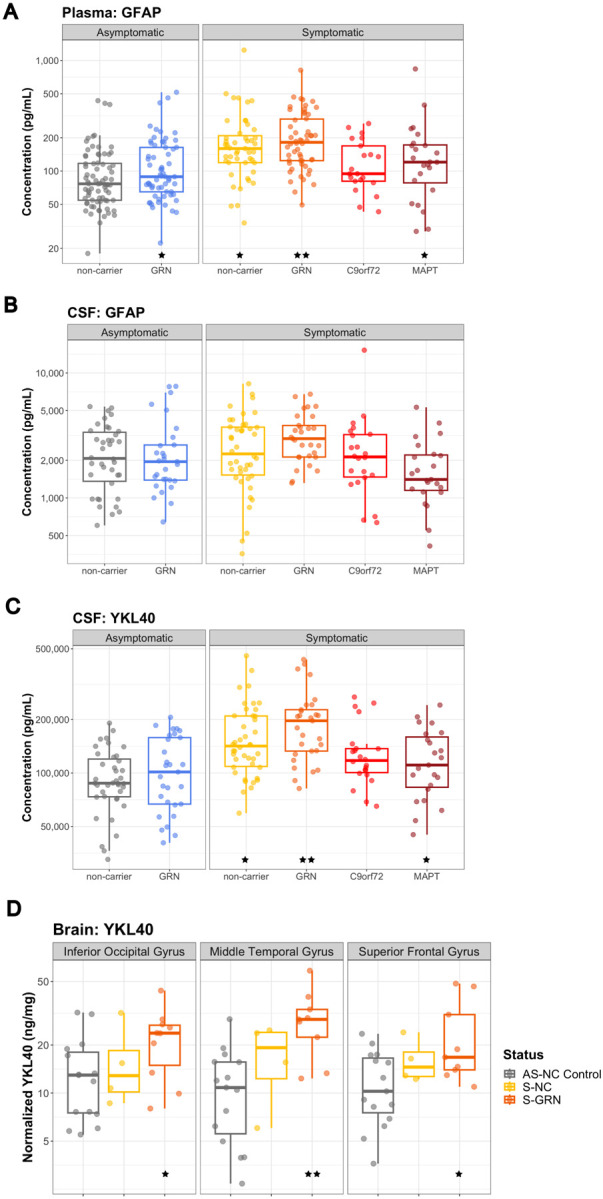
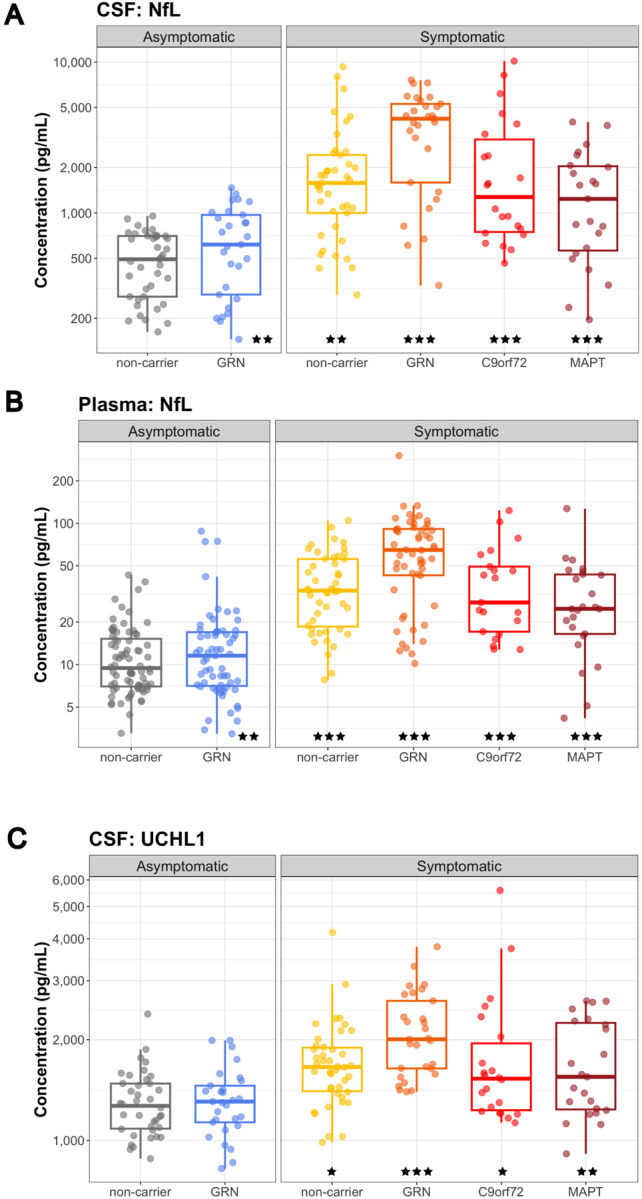
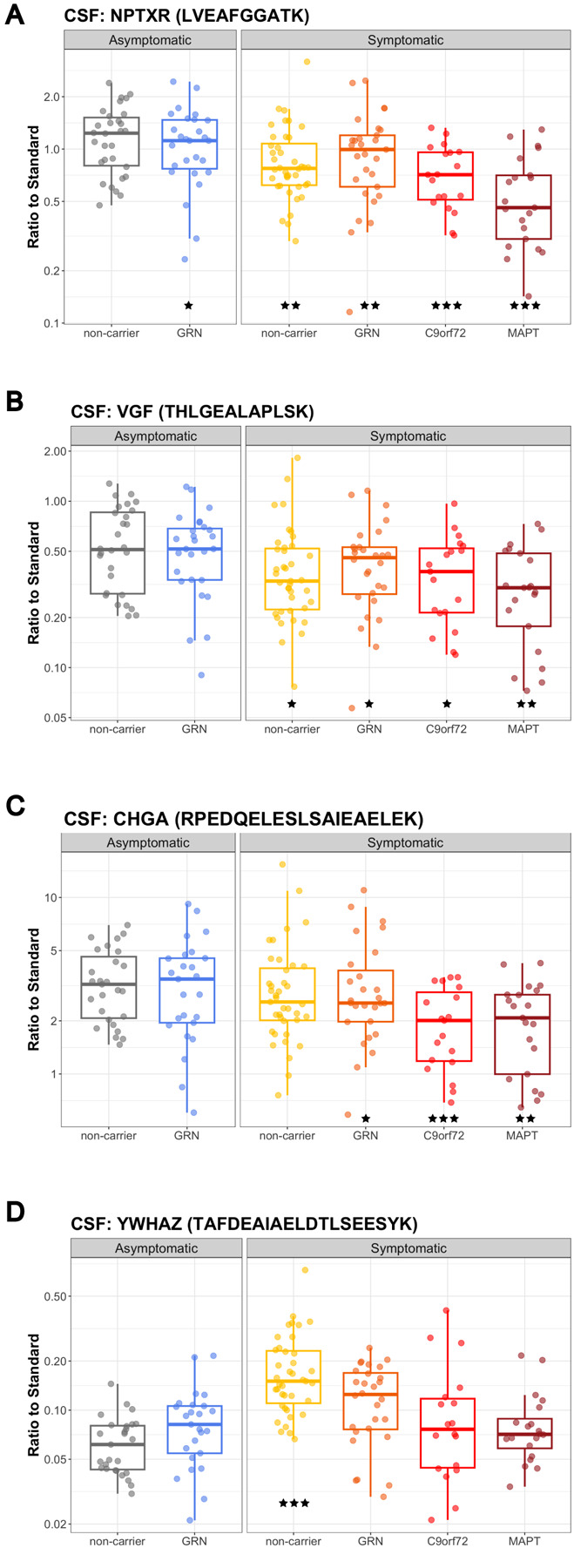
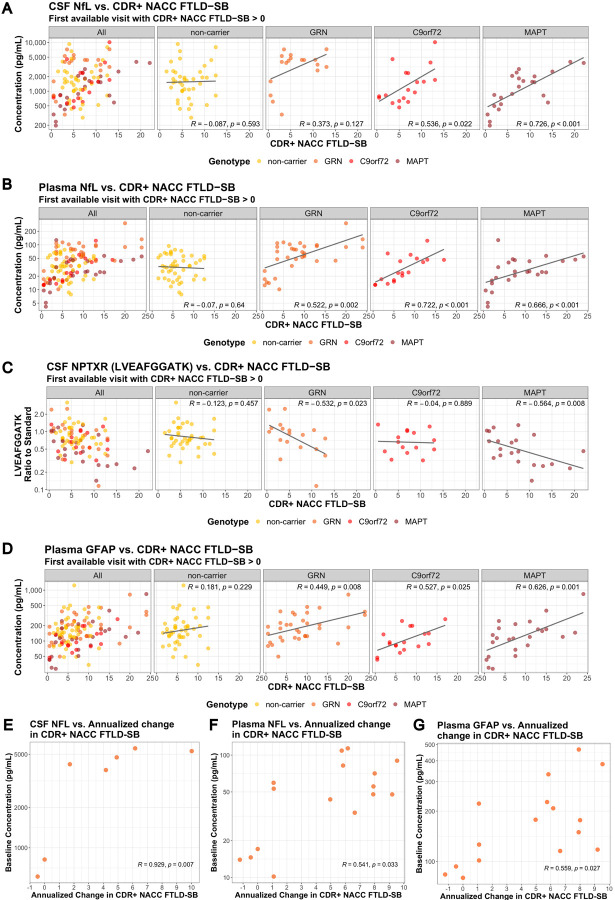
Results: We confirmed glucosylsphingosine (GlcSph), a lysosomal biomarker regulated by progranulin, was elevated in the plasma from GRN mutation carriers, both symptomatic and asymptomatic. GlcSph and other lysosomal biomarkers such as ganglioside GM2 and globoside GB3 were increased in the disease affected SFG and MTG regions from sporadic FTD and symptomatic GRN mutation carriers, but not in the IOG, compared to the same brain regions from controls. The glial biomarkers GFAP in plasma and YKL40 in CSF were elevated in asymptomatic GRN carriers, and all symptomatic groups, except the symptomatic C9orf72 mutation group. YKL40 was also increased in SFG and MTG regions from sporadic FTD and symptomatic GRN mutation carriers. Neuronal injury and degeneration biomarkers NfL in CSF and plasma, and UCHL1 in CSF were elevated in patients with all forms of FTD. Synaptic biomarkers NPTXR, NPTX1/2, and VGF were reduced in CSF from patients with all forms of FTD, with the most pronounced reductions observed in symptomatic MAPT mutation carriers. Furthermore, we demonstrated plasma NfL was significantly positively correlated with disease severity as measured by CDR+NACC FTLD SB in genetic forms of FTD and CSF NPTXR was significantly negatively correlated with CDR+NACC FTLD SB in symptomatic GRN and MAPT mutation carriers.
Conclusions: In conclusion, our comprehensive investigation replicated alterations in biofluid biomarkers indicative of lysosomal function, glial activation, synaptic and neuronal health across sporadic and genetic forms of FTD and unveiled novel insights into the dysregulation of these biomarkers within brain tissues from patients with GRN mutations. The observed correlations between biomarkers and disease severity open promising avenues for prognostic applications and for indicators of drug efficacy in clinical trials. Our data also implicated a complicated relationship between biofluid and tissue biomarker changes and future investigations should delve into the mechanistic underpinnings of these biomarkers, which will serve as a foundation for the development of targeted therapeutics for FTD.
Keywords: C9orf72; Frontotemporal dementia; GFAP; GRN; MAPT; NPTXR; NTPX; NfL; YKL-40; biomarker; glial; lysosomal; sporadic FTD; synaptic.
Figures
Similar articles
-
Differential impairment of cerebrospinal fluid synaptic biomarkers in the genetic forms of frontotemporal dementia.Alzheimers Res Ther. 2022 Aug 31;14(1):118. doi: 10.1186/s13195-022-01042-3. Alzheimers Res Ther. 2022. PMID: 36045450 Free PMC article.
-
Comparison of clinical rating scales in genetic frontotemporal dementia within the GENFI cohort.J Neurol Neurosurg Psychiatry. 2022 Feb;93(2):158-168. doi: 10.1136/jnnp-2021-326868. Epub 2021 Aug 5. J Neurol Neurosurg Psychiatry. 2022. PMID: 34353857 Free PMC article.
-
Cerebrospinal Fluid YKL-40 and Chitotriosidase Levels in Frontotemporal Dementia Vary by Clinical, Genetic and Pathological Subtype.Dement Geriatr Cogn Disord. 2020;49(1):56-76. doi: 10.1159/000506282. Epub 2020 Apr 28. Dement Geriatr Cogn Disord. 2020. PMID: 32344399 Free PMC article.
-
An update on genetic frontotemporal dementia.J Neurol. 2019 Aug;266(8):2075-2086. doi: 10.1007/s00415-019-09363-4. Epub 2019 May 22. J Neurol. 2019. PMID: 31119452 Free PMC article. Review.
-
Blood-Based Biomarkers in Frontotemporal Dementia: A Narrative Review.Int J Mol Sci. 2024 Nov 4;25(21):11838. doi: 10.3390/ijms252111838. Int J Mol Sci. 2024. PMID: 39519389 Free PMC article. Review.
References
-
- Boeve B. F., Boxer A. L., Kumfor F., Pijnenburg Y. & Rohrer J. D. Advances and controversies in frontotemporal dementia: diagnosis, biomarkers, and therapeutic considerations. Lancet Neurol. 21, 258–272 (2022). - PubMed
-
- Baker M. et al. Mutations in progranulin cause tau-negative frontotemporal dementia linked to chromosome 17. Nature 442, 916–919 (2006). - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous