

This is a preprint.
Quantifying the impact of cascade inequalities: a modelling study on the prevention impacts of antiretroviral therapy scale-up in Eswatini
- PMID: 38405846
- PMCID: PMC10889039
- DOI: 10.1101/2024.02.16.24302584
Quantifying the impact of cascade inequalities: a modelling study on the prevention impacts of antiretroviral therapy scale-up in Eswatini
Abstract
Background: Inequalities in the antiretroviral therapy (ART) cascade across subpopulations remain an ongoing challenge in the global HIV response. Eswatini achieved the UNAIDS 95-95-95 targets by 2020, with differentiated programs to minimize inequalities across subpopulations, including for female sex workers (FSW) and their clients. We sought to estimate additional HIV infections expected in Eswatini if cascade scale-up had not been equal, and under which epidemic conditions these inequalities could have the largest influence.
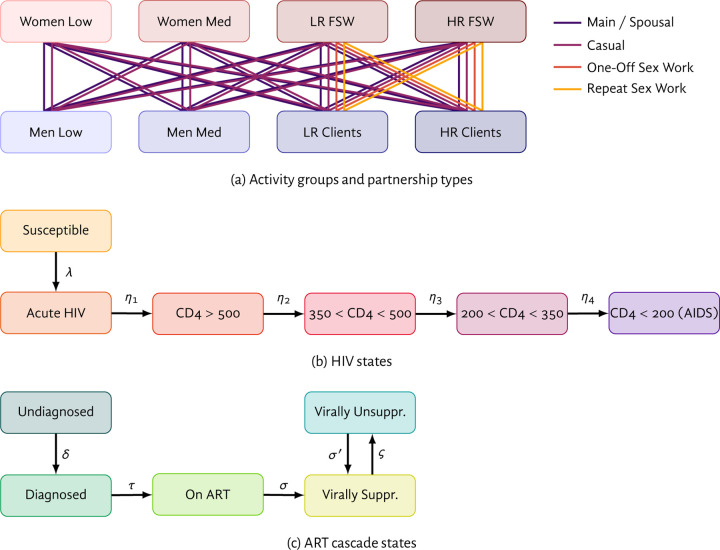
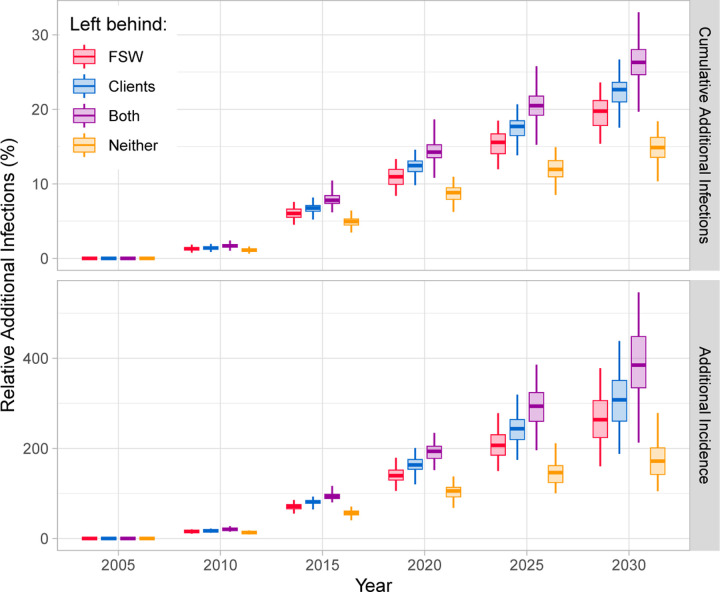
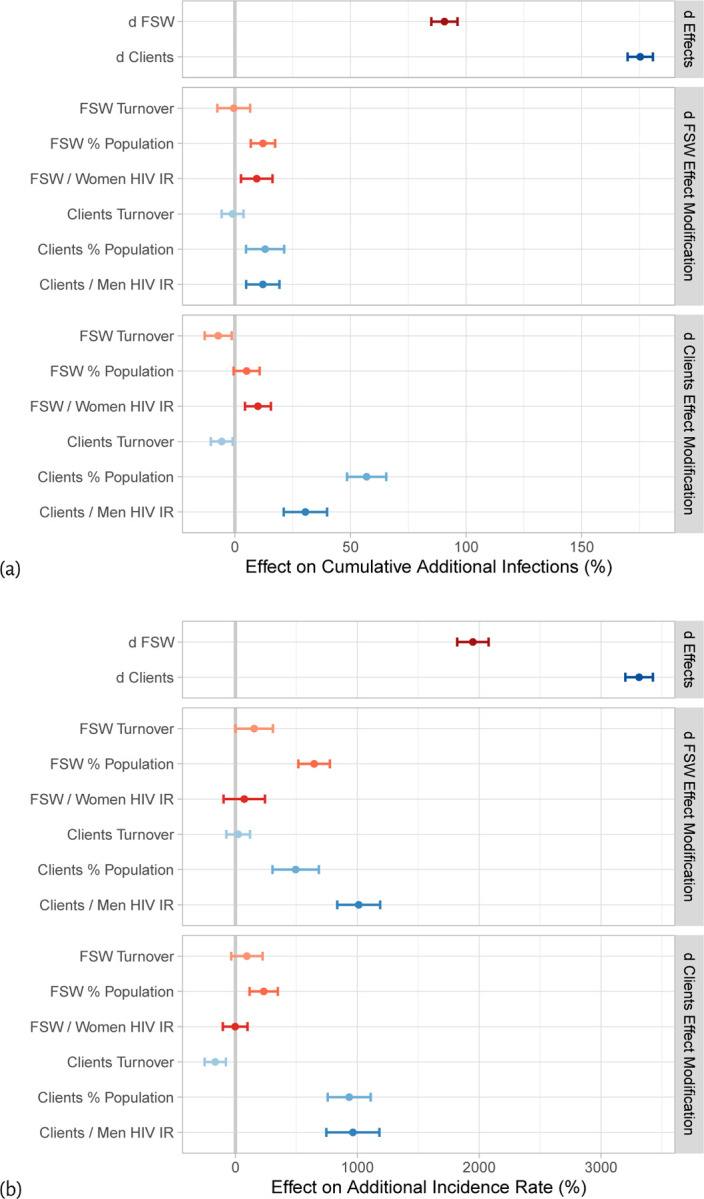
Methods: Drawing on population-level and FSW-specific surveys in Eswatini, we developed a compartmental model of heterosexual HIV transmission which included eight subpopulations and four sexual partnership types. We calibrated the model to stratified HIV prevalence, incidence, and ART cascade data. Taking observed cascade scale-up in Eswatini as the base-case-reaching 95-95-95 in the overall population by 2020-we defined four counterfactual scenarios in which the population overall reached 80-80-90 by 2020, but where FSW, clients, both, or neither were disproportionately left behind, reaching only 60-40-80. We quantified relative additional cumulative HIV infections by 2030 in counterfactual vs base-case scenarios. We further estimated linear effects of viral suppression gap among FSW and clients on additional infections by 2030, plus effect modification by FSW/client population sizes, rates of turnover, and HIV prevalence ratios.
Results: Compared with the base-case scenario, leaving behind neither FSW nor their clients led to the fewest additional infections by 2030: median (95% credible interval) 14.9 (10.4, 18.4)% vs 26.3 (19.7, 33.0)% if both were left behind-a 73 (40, 149)% increase. The effect of lower cascade on additional infections was larger for clients vs FSW, and both effects increased with population size and relative HIV incidence.
Conclusions: Inequalities in the ART cascade across subpopulations can undermine the anticipated prevention impacts of cascade scale-up. As Eswatini has shown, addressing inequalities in the ART cascade, particularly those that intersect with high transmission risk, could maximize incidence reductions from cascade scale-up.
Keywords: HIV; antiretroviral therapy; healthcare disparities; mathematical model; sex work.
Figures
Similar articles
-
The effect of 90-90-90 on HIV-1 incidence and mortality in eSwatini: a mathematical modelling study.Lancet HIV. 2020 May;7(5):e348-e358. doi: 10.1016/S2352-3018(19)30436-9. Epub 2020 Feb 13. Lancet HIV. 2020. PMID: 32061317 Free PMC article.
-
Population-level impact of an accelerated HIV response plan to reach the UNAIDS 90-90-90 target in Côte d'Ivoire: Insights from mathematical modeling.PLoS Med. 2017 Jun 15;14(6):e1002321. doi: 10.1371/journal.pmed.1002321. eCollection 2017 Jun. PLoS Med. 2017. PMID: 28617810 Free PMC article.
-
Strengthening the scale-up and uptake of effective interventions for sex workers for population impact in Zimbabwe.J Int AIDS Soc. 2019 Jul;22 Suppl 4(Suppl Suppl 4):e25320. doi: 10.1002/jia2.25320. J Int AIDS Soc. 2019. PMID: 31328445 Free PMC article.
-
Changing Dynamics of HIV Transmission in Côte d'Ivoire: Modeling Who Acquired and Transmitted Infections and Estimating the Impact of Past HIV Interventions (1976-2015).J Acquir Immune Defic Syndr. 2017 Aug 15;75(5):517-527. doi: 10.1097/QAI.0000000000001434. J Acquir Immune Defic Syndr. 2017. PMID: 28471837 Free PMC article.
-
Risk heterogeneity in compartmental HIV transmission models of ART as prevention in Sub-Saharan Africa: A scoping review.Epidemics. 2022 Sep;40:100608. doi: 10.1016/j.epidem.2022.100608. Epub 2022 Jul 8. Epidemics. 2022. PMID: 35843152
References
-
- UNAIDS. The path that ends AIDS: 2023 UNAIDS Global AIDS Update. Geneva, Switzerland, 2023.
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous