

This is a preprint.
Comparison of Infectious Complications with BCMA-directed Therapies in Multiple Myeloma
- PMID: 38405866
- PMCID: PMC10889082
- DOI: 10.21203/rs.3.rs-3911922/v1
Comparison of Infectious Complications with BCMA-directed Therapies in Multiple Myeloma
Update in
-
Comparison of infectious complications with BCMA-directed therapies in multiple myeloma.Blood Cancer J. 2024 May 31;14(1):88. doi: 10.1038/s41408-024-01043-5. Blood Cancer J. 2024. PMID: 38821925 Free PMC article.
Abstract
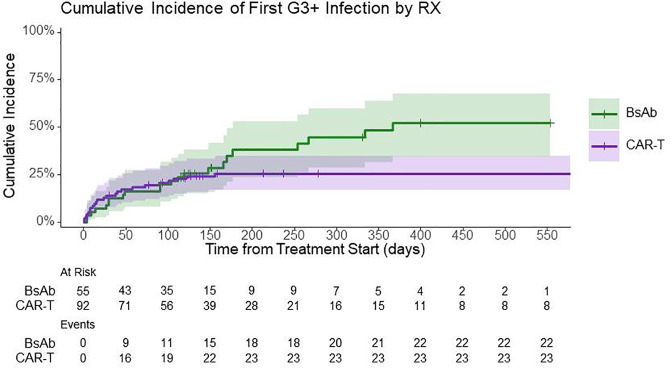
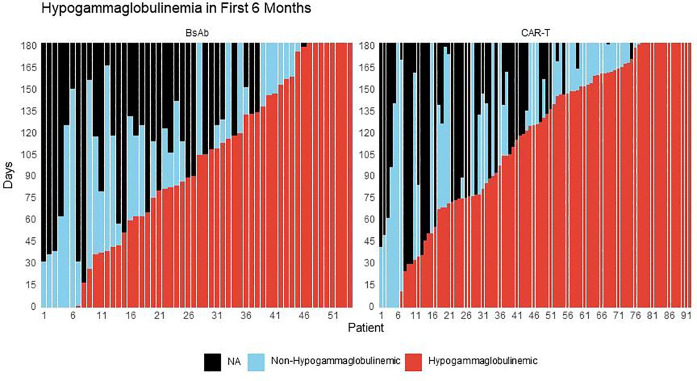
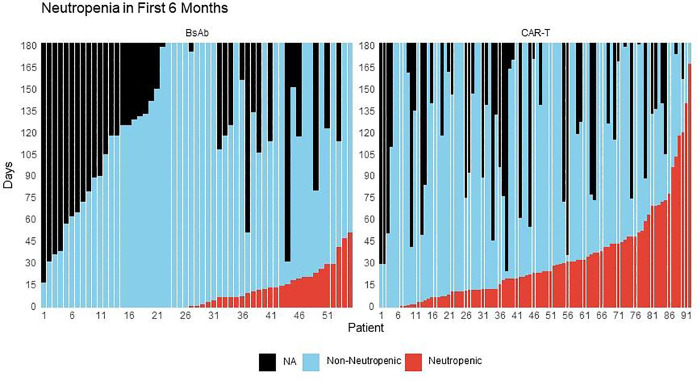
B-cell-maturation-antigen (BCMA)-directed therapies are highly active for multiple myeloma, but infections are emerging as a major challenge. In this retrospective, single-center analysis we evaluated infectious complications after BCMA-targeted chimeric-antigen-receptor T-cell therapy (CAR-T), bispecific-antibodies (BsAb) and antibody-drug-conjugates (ADC). The primary endpoint was severe (grade ≥ 3) infection incidence. Amongst 256 patients, 92 received CAR-T, 55 BsAb and 109 ADC. The incidence of severe infections was higher with BsAb (40%) than CAR-T (26%) or ADC (8%), including grade 5 infections (7% vs 0% vs 0%, respectively). Comparing T-cell redirecting therapies, the incidence rate of severe infections was significantly lower with CAR-T compared to BsAb at 1-year (incidence-rate-ratio [IRR] = 0.43, 95%CI 0.25-0.76, P = 0.004). During periods of treatment-emergent hypogammaglobulinemia, BsAb recipients had higher infection rates (IRR:2.27, 1.31-3.98, P = 0.004) and time to severe infection (HR 2.04, 1.05-3.96, P = 0.036) than their CAR-T counterparts. During periods of non-neutropenia, CAR-T recipients had a lower risk (HR 0.44, 95%CI 0.21-0.93, P = 0.032) and incidence rate (IRR:0.32, 95% 0.17-0.59, P < 0.001) of severe infections than BsAb. In conclusion, we observed an overall higher and more persistent risk of severe infections with BsAb. Our results also suggest a higher infection risk during periods of hypogammaglobulinemia with BsAb, and with neutropenia in CAR-T recipients.
Conflict of interest statement
COMPETING INTERESTS Tala Shekarkhand reports honoraria from Genentech; David J Chung receives research funding from Genentech; Heather J Landau has served as a paid consultant for Takeda, Genzyme, Janssen, Karyopharm, Pfizer, Celgene, Caelum Biosciences, and has received research support from Takeda; Oscar B Lahoud reports serving on Advisory Board for MorphoSys Inc., Kite, Daiichi Sankyo Inc., Incyte; Consulting for: Incyte; Michael Scordo served as a paid consultant for McKinsey & Company, Angiocrine Bioscience, Inc., and Omeros Corporation; received research funding from Angiocrine Bioscience, Inc., Omeros Corporation, and Amgen, Inc.; served on ad hoc advisory boards for Kite – A Gilead Company; and received honoraria from i3Health, Medscape, and CancerNetwork for CME-related activity; Gunjan Shah reports research funding from Janssen, Amgen, BMS, Beyond Spring, and serves on the Data Safety Monitoring Board for ArcellX. G.S. research funding to the institution from Janssen, Amgen, BMS, Beyond Spring, and GPCR, and on DSMB for ArcellX; Hani Hassoun reports grants from Celgene, Takeda, and Janssen, outside the submitted work; Neha Korde reports research funding through Amgen and participates in advisory board with Medimmune; Urvi Shah reports personal fees from Physicians Educations Resources; grants and other from Celgene/Bristol Myers Squibb; other from Janssen; and grants from Parker Institute for Cancer Immunotherapy and Myeloma Crowd, outside the submitted work; Carlyn Tan: reports research funding from Janssen and personal fees from Physician Educations Resource; Malin Hultcrantz: reports research funding from Amgen, Daiichi Sankyo, GlaxoSmithKline; has received honoraria for consultancy/participated in advisory boards for Curio Science LLC, Intellisphere LLC, Bristol Myer Squibb, and GlaxoSmithKline; Sergio A. Giralt reports personal fees from and an advisory role (scientific advisory board) in Actinium, Celgene, Bristol Myers Squibb, Sanofi, Amgen, Pfizer, GlaxoSmithKline, JAZZ, Janssen, Omeros, Takeda, and Kite, outside the submitted work; Saad Z Usmani reports grants and personal fees from AbbVie, 404 Amgen, BMS, Celgene, GSK, Janssen, Merck, MundiPharma, Oncopeptides, 405 Pharmacyclics, Sanofi, Seattle Genetics, SkylineDX, and Takeda; Sham Mailankody received consulting fees from Evicore, Optum, BioAscend, Janssen Oncology, Bristol Myers Squibb, AbbVie, ECor1, Galapagos, and Legend Biotech. Memorial Sloan Kettering Cancer Center receives research funding from the NCI, Janssen Oncology, Bristol Myers Squibb, Allogene Therapeutics, Fate Therapeutics, and Takeda Oncology for research led by Sham Mailankody. Sham Mailankody received honoraria from OncLive, Physician Education Resource, MJH Life Sciences, and Plexus Communications; Alexander M Lesokhin reports grants from Bristol Myers Squibb; personal fees from Trillium Therapeutics; grants, personal fees and non-financial support from Pfizer; and grants and personal fees from Janssen and Arcellx, outside the submitted work. A.M.L also has a patent US20150037346A1 with royalties paid.
Figures
References
-
- Novak AJ, Darce JR, Arendt BK, Harder B, Henderson K, Kindsvogel W, et al. Expression of BCMA, TACI, and BAFF-R in multiple myeloma: a mechanism for growth and survival. Blood. 2004;103(2):689–94. - PubMed
-
- Martin T, Usmani SZ, Berdeja JG, Agha M, Cohen AD, Hari P, et al. Ciltacabtagene Autoleucel, an Anti–B-cell Maturation Antigen Chimeric Antigen Receptor T-Cell Therapy, for Relapsed/Refractory Multiple Myeloma: CARTITUDE-1 2-Year Follow-Up. Journal of Clinical Oncology. 2022:JCO.22.00842. - PMC - PubMed
-
- Munshi NC, Anderson LD, Shah N, Madduri D, Berdeja J, Lonial S, et al. Idecabtagene Vicleucel in Relapsed and Refractory Multiple Myeloma. New England Journal of Medicine. 2021;384(8):705–16. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
