

Biliary Disease in a Tertiary Care Hospital: A Review of Clinical and Radiological Burden
- PMID: 38406075
- PMCID: PMC10893906
- DOI: 10.7759/cureus.52927
Biliary Disease in a Tertiary Care Hospital: A Review of Clinical and Radiological Burden
Abstract
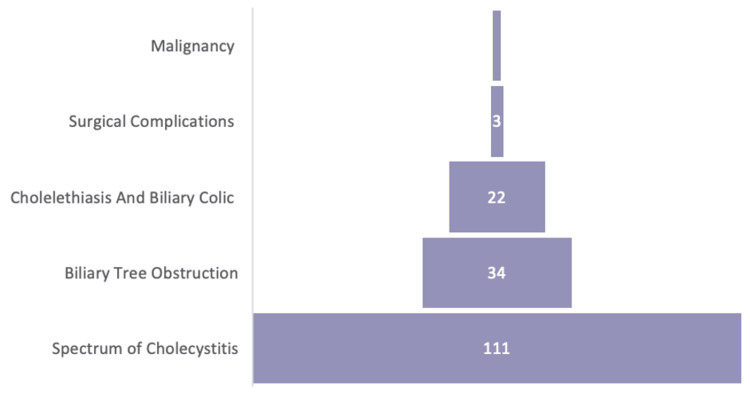
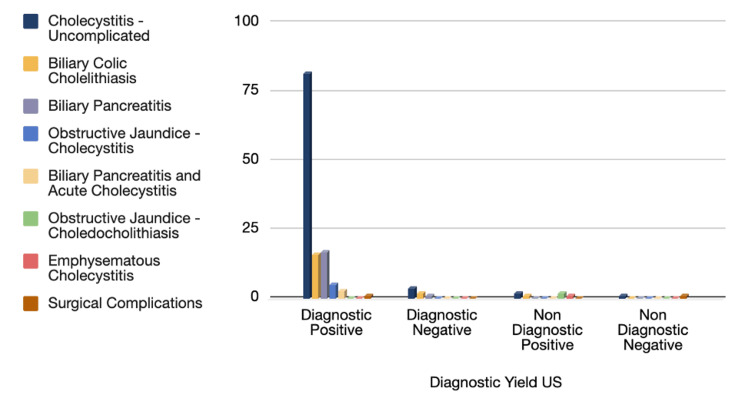
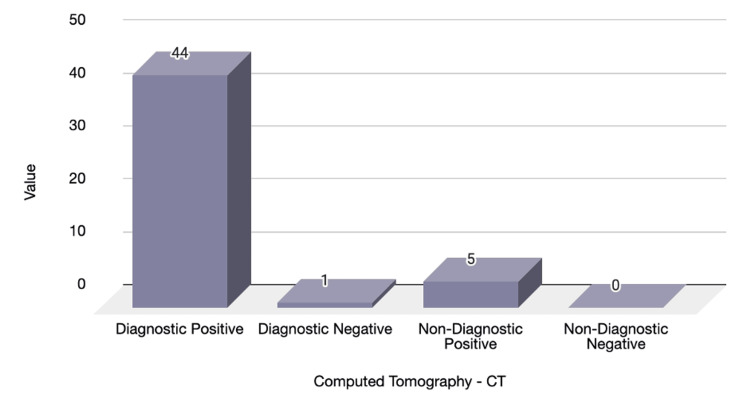
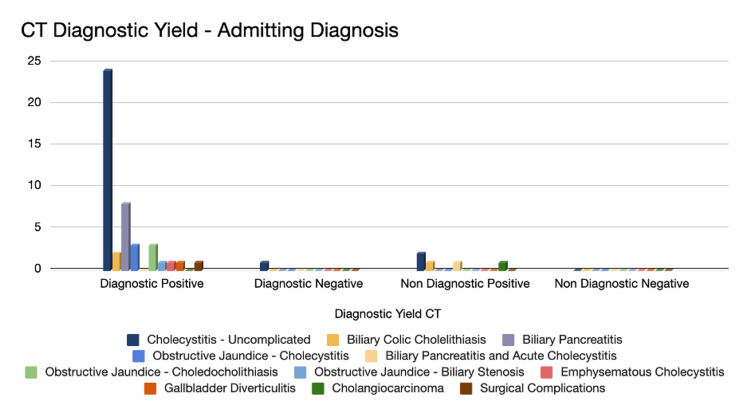
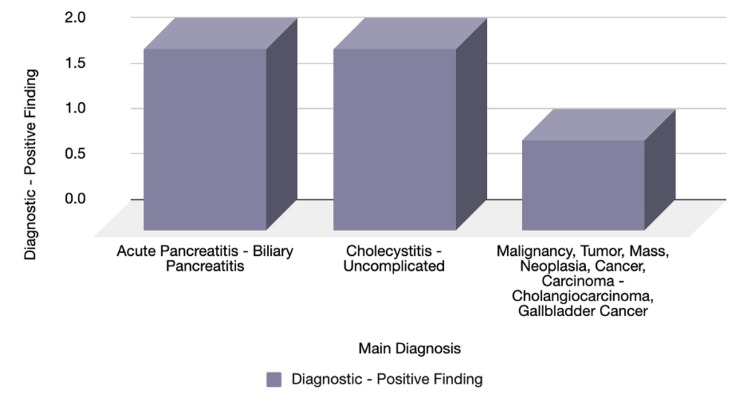
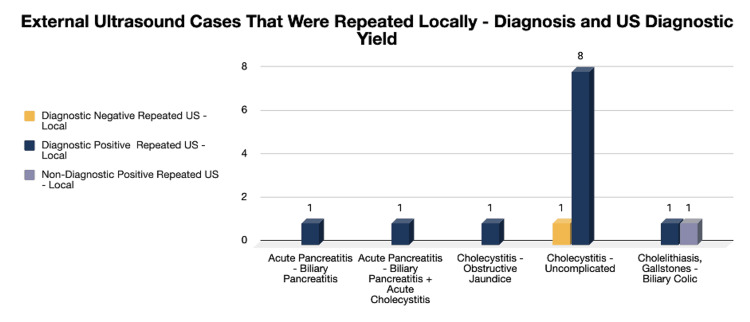
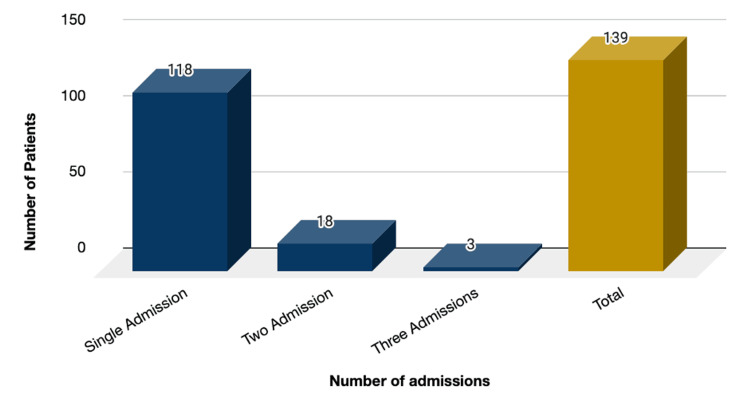
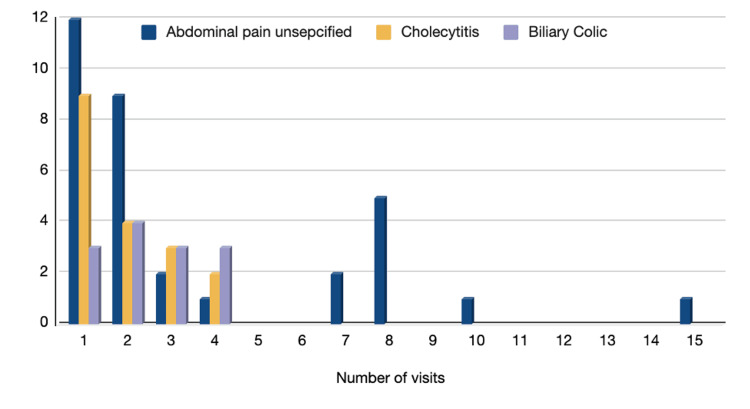
Introduction Gallbladder disease accounts for a significant percentage of surgical admissions per year. A review of these cases was done to assess their hospital impact with an evaluation of the efficacy of radiological modalities in terms of evaluation, ideal use, and clinical application. Therefore, this study aims to review the demographics of the disease, the diagnostic yield of radiological modalities, and the overall outcome in regards to the hospital policies and medical services provided in hopes of achieving suitable clinical pathways, increasing the efficiency of gallbladder disease assessment, and limiting unwarranted investigations. Methods This is a single-center, retrospective study that included all the surgical emergency admissions from January 1st to December 31st 2018, in the Salmaniya Medical Complex, Kingdom of Bahrain. A total sample of 163 emergency admissions (cases) was selected from those aged 14 and older with documented biliary stones or biliary-related disease. A review of radiological modalities for diagnosis included plain radiographs (AXR, CXR), US abdomen, CT scans, and MRCP/MRI, which were then correlated with histopathological findings confirming the presence of gallstone disease. In addition to evaluating readmissions and emergency visits in terms of hospital burden. Results One hundred and sixty-three (10.44%) of 1,562 surgical admission cases in 2018 were diagnosed with biliary tree disease (76 males, 87 females). A total of 419 different radiological investigations were requested in 161 of the cases evaluated: 53.7% of plain radiographs (AXR, CXR), 33.2% of US abdomen, 11.9% of CT scan, and 1.2% of MRCP/MRI. Ultrasound showed a sensitivity of 48.72% and a specificity of 100%, while CT scan sensitivity was 57.14% and a specificity of 100% when it came to detecting gallstones and gallbladder-related disease. Plain radiographs add no direct benefit to diagnosing biliary disease. Conclusion Gallbladder disease is very prevalent with a wide array of disease entities, requiring radiological assistance in diagnosis. Ultrasound is the ideal modality for the diagnosis of biliary disease due to its ease of use and availability; it has high sensitivity and specificity, and it can be complemented by other modalities such as CT scans and MRCP/MRI when it comes to assessing for complications. On the other hand, plain radiographs have no significant value in the detection of gallbladder-related disease, and their utilization should be limited to emergency cases with high clinical suspicion.
Keywords: biliary pancreatitis; cholecystitis; cholelithiasis; hospital burden; ultrasound imaging.
Copyright © 2024, Mahdi et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures




Similar articles
-
Accuracy of magnetic resonance cholangiography compared to operative endoscopy in detecting biliary stones, a single center experience and review of literature.World J Radiol. 2015 Apr 28;7(4):70-8. doi: 10.4329/wjr.v7.i4.70. World J Radiol. 2015. PMID: 25918584 Free PMC article.
-
A Review of Radiological Investigations in Cases of Acute Appendicitis in a Tertiary Care Hospital.Cureus. 2023 Mar 30;15(3):e36916. doi: 10.7759/cureus.36916. eCollection 2023 Mar. Cureus. 2023. PMID: 37128517 Free PMC article.
-
The diagnostic utility of HASTE MRI in the evaluation of acute cholecystitis. Half-Fourier acquisition single-shot turbo SE.J Comput Assist Tomogr. 1998 Jul-Aug;22(4):638-42. doi: 10.1097/00004728-199807000-00025. J Comput Assist Tomogr. 1998. PMID: 9676460 Clinical Trial.
-
Advancements in Cholelithiasis Diagnosis: A Systematic Review of Machine Learning Applications in Imaging Analysis.Cureus. 2024 Aug 8;16(8):e66453. doi: 10.7759/cureus.66453. eCollection 2024 Aug. Cureus. 2024. PMID: 39247002 Free PMC article. Review.
-
Multimodality Imaging, including Dual-Energy CT, in the Evaluation of Gallbladder Disease.Radiographics. 2018 Jan-Feb;38(1):75-89. doi: 10.1148/rg.2018170076. Radiographics. 2018. PMID: 29320323 Review.
References
-
- Gallstones: Watch and wait, or intervene? Ibrahim M, Sarvepalli S, Morris-Stiff G, et al. Cleve Clin J Med. 2018;85:323–331. - PubMed
LinkOut - more resources
Full Text Sources