

Chronic intermittent hypoxia-induced hypertension: the impact of sex hormones
- PMID: 38406843
- PMCID: PMC11381015
- DOI: 10.1152/ajpregu.00258.2023
Chronic intermittent hypoxia-induced hypertension: the impact of sex hormones
Abstract
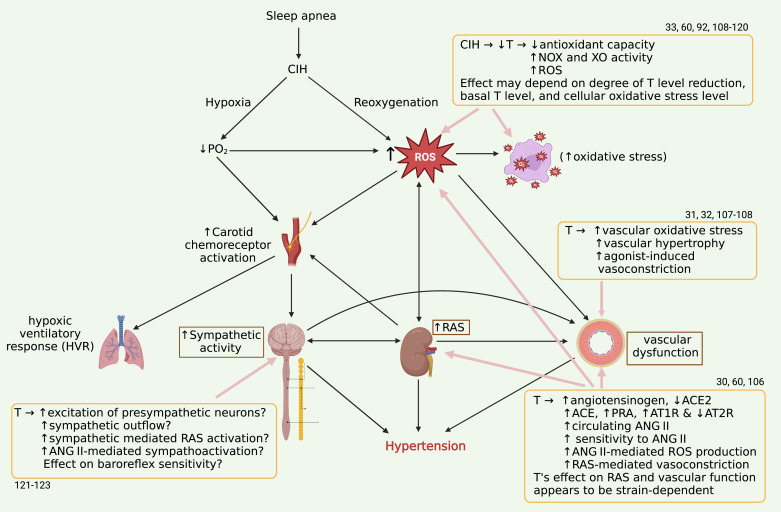
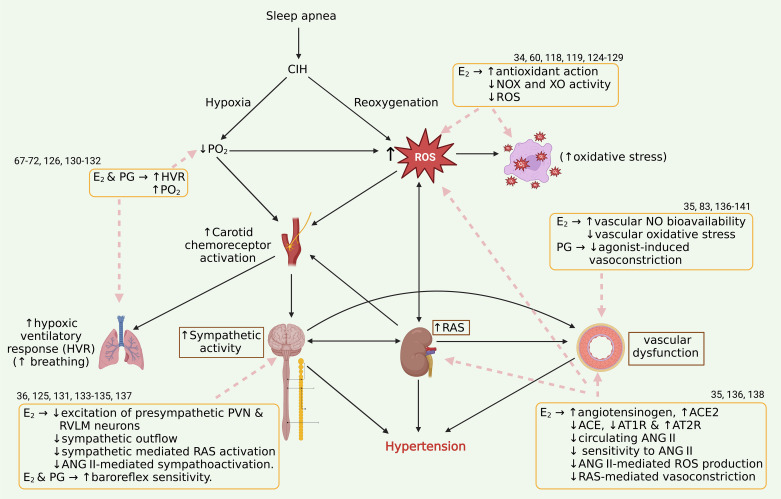
Obstructive sleep apnea, a common form of sleep-disordered breathing, is characterized by intermittent cessations of breathing that reduce blood oxygen levels and contribute to the development of hypertension. Hypertension is a major complication of obstructive sleep apnea that elevates the risk of end-organ damage. Premenopausal women have a lower prevalence of obstructive sleep apnea and cardiovascular disease than men and postmenopausal women, suggesting that sex hormones play a role in the pathophysiology of sleep apnea-related hypertension. The lack of protection in men and postmenopausal women implicates estrogen and progesterone as protective agents but testosterone as a permissive agent in sleep apnea-induced hypertension. A better understanding of how sex hormones contribute to the pathophysiology of sleep apnea-induced hypertension is important for future research and possible hormone-based interventions. The effect of sex on the pathophysiology of sleep apnea and associated intermittent hypoxia-induced hypertension is of important consideration in the screening, diagnosis, and treatment of the disease and its cardiovascular complications. This review summarizes our current understanding of the impact of sex hormones on blood pressure regulation in sleep apnea with a focus on sex differences.
Keywords: estrogens; hypertension; sleep apnea; sympathetic nervous system; testosterone.
Conflict of interest statement
No conflicts of interest, financial or otherwise, are declared by the authors.
Figures
References
-
- Guo WB, Liu YP, Xu HH, Meng LL, Zhu HM, Wu HM, Guan J, Yi HL, Yin SK. [Obstructive sleep apnea and metabolic syndrome: an association study based on a large sample clinical database]. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi 56: 1263–1269, 2021. doi: 10.3760/cma.j.cn115330-20210531-00314. - DOI - PubMed
-
- Su X, Han J, Gao Y, He Z, Zhao Z, Lin J, Guo J, Chen K, Gao Y, Liu L. [Correlation of obstructive sleep apnea with components of metabolic syndrome and implications for long-term adverse cardiovascular risk in elderly patients]. Nan Fang Yi Ke Da Xue Xue Bao 41: 1592–1599, 2021. doi: 10.12122/j.issn.1673-4254.2021.11.01. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical