

Validation of a screening panel for pediatric metabolic dysfunction-associated steatotic liver disease using metabolomics
- PMID: 38407264
- PMCID: PMC10898657
- DOI: 10.1097/HC9.0000000000000375
Validation of a screening panel for pediatric metabolic dysfunction-associated steatotic liver disease using metabolomics
Abstract
Background: Metabolic dysfunction-associated steatotic liver disease (MASLD), formerly known as NAFLD, is the most common liver disease in children. Liver biopsy remains the gold standard for diagnosis, although more efficient screening methods are needed. We previously developed a novel NAFLD screening panel in youth using machine learning applied to high-resolution metabolomics and clinical phenotype data. Our objective was to validate this panel in a separate cohort, which consisted of a combined cross-sectional sample of 161 children with stored frozen samples (75% male, 12.8±2.6 years of age, body mass index 31.0±7.0 kg/m2, 81% with MASLD, 58% Hispanic race/ethnicity).
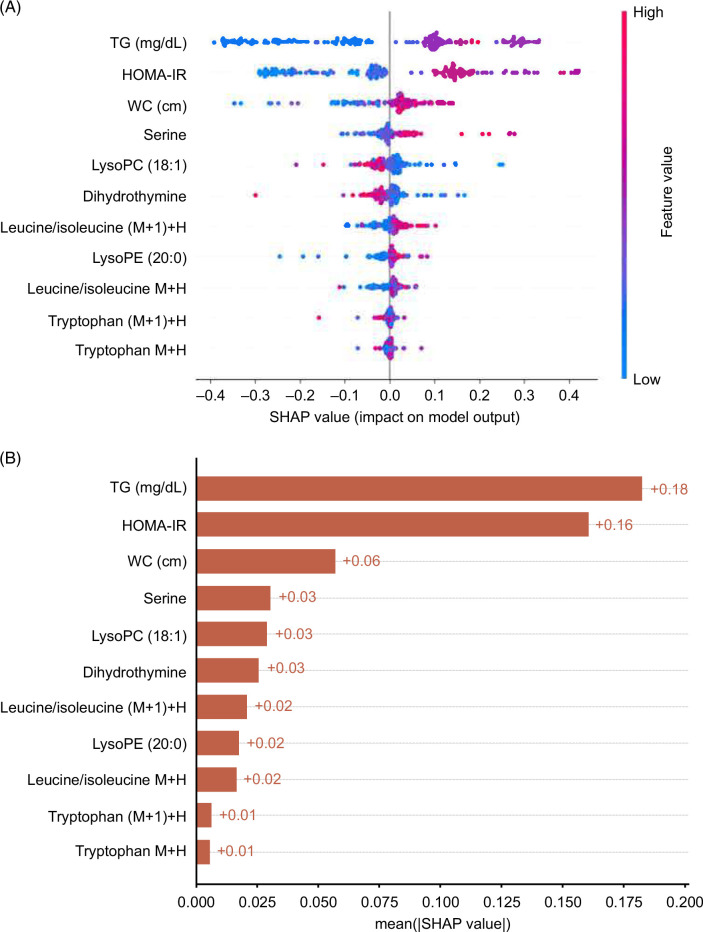
Methods: Clinical data were collected from all children, and high-resolution metabolomics was performed using their fasting serum samples. MASLD was assessed by MRI-proton density fat fraction or liver biopsy and cardiometabolic factors. Our previously developed panel included waist circumference, triglycerides, whole-body insulin sensitivity index, 3 amino acids, 2 phospholipids, dihydrothymine, and 2 unknowns. To improve feasibility, a simplified version without the unknowns was utilized in the present study. Since the panel was modified, the data were split into training (67%) and test (33%) sets to assess the validity of the panel.
Results: Our present highest-performing modified model, with 4 clinical variables and 8 metabolomics features, achieved an AUROC of 0.92, 95% sensitivity, and 80% specificity for detecting MASLD in the test set.
Conclusions: Therefore, this panel has promising potential for use as a screening tool for MASLD in youth.
Copyright © 2024 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Association for the Study of Liver Diseases.
Conflict of interest statement
Miriam B. Vos serves as a consultant to Boehringer Ingelheim, Novo Nordisk, Eli Lilly, Intercept, Takeda, and Alberio. She has stock or stock options in Thiogenesis and Tern Pharmaceuticals. Her institution has received research grants (or in-kind research services) from Target Real World Evidence, Quest, Labcorp, and Sonic Incytes Medical Corp. The remaining authors have no conflicts to report.
Figures

References
-
- Rinella ME, Lazarus JV, Ratziu V, Francque SM, Sanyal AJ, Kanwal F, et al. . A multi-society Delphi consensus statement on new fatty liver disease nomenclature. Ann Hepatol. 2023;29:101133. - PubMed
-
- Draijer L, Benninga M, Koot B. Pediatric NAFLD: an overview and recent developments in diagnostics and treatment. Expert Rev Gastroenterol Hepatol. 2019;13:447–61. - PubMed
-
- Reinehr T, Schmidt C, Toschke AM, Andler W. Lifestyle intervention in obese children with non-alcoholic fatty liver disease: 2-year follow-up study. Arch Dis Child. 2009;94:437–42. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
