

First-in-Human Study of the Ataxia Telangiectasia and Rad3-Related (ATR) Inhibitor Tuvusertib (M1774) as Monotherapy in Patients with Solid Tumors
- PMID: 38407317
- PMCID: PMC11094421
- DOI: 10.1158/1078-0432.CCR-23-2409
First-in-Human Study of the Ataxia Telangiectasia and Rad3-Related (ATR) Inhibitor Tuvusertib (M1774) as Monotherapy in Patients with Solid Tumors
Abstract
Purpose: Tuvusertib (M1774) is a potent, selective, orally administered ataxia telangiectasia and Rad3-related (ATR) protein kinase inhibitor. This first-in-human study (NCT04170153) evaluated safety, tolerability, maximum tolerated dose (MTD), recommended dose for expansion (RDE), pharmacokinetics (PK), pharmacodynamics (PD), and preliminary efficacy of tuvusertib monotherapy.
Patients and methods: Ascending tuvusertib doses were evaluated in 55 patients with metastatic or locally advanced unresectable solid tumors. A safety monitoring committee determined dose escalation based on PK, PD, and safety data guided by a Bayesian 2-parameter logistic regression model. Molecular responses (MR) were assessed in circulating tumor DNA samples.
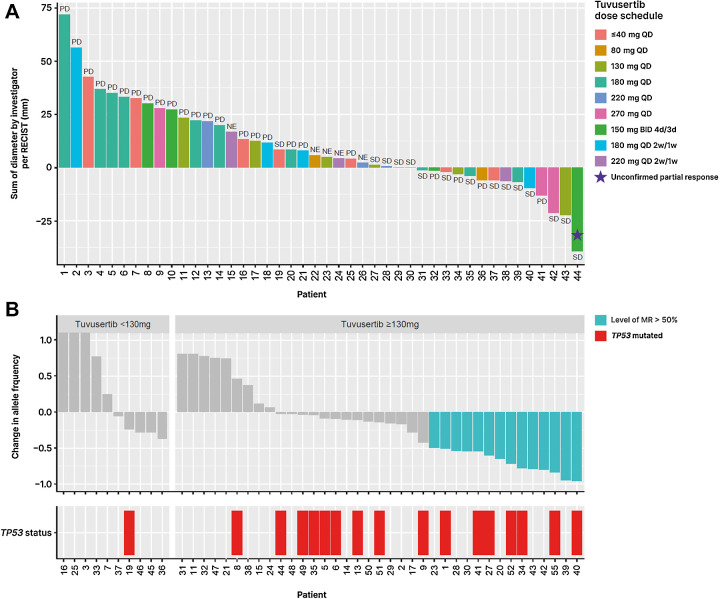
Results: Most common grade ≥3 treatment-emergent adverse events were anemia (36%), neutropenia, and lymphopenia (both 7%). Eleven patients experienced dose-limiting toxicities, most commonly grade 2 (n = 2) or 3 (n = 8) anemia. No persistent effects on blood immune cell populations were observed. The RDE was 180 mg tuvusertib QD (once daily), 2 weeks on/1 week off treatment, which was better tolerated than the MTD (180 mg QD continuously). Tuvusertib median time to peak plasma concentration ranged from 0.5 to 3.5 hours and mean elimination half-life from 1.2 to 5.6 hours. Exposure-related PD analysis suggested maximum target engagement at ≥130 mg tuvusertib QD. Tuvusertib induced frequent MRs in the predicted efficacious dose range; MRs were enriched in patients with radiological disease stabilization, and complete MRs were detected for mutations in ARID1A, ATRX, and DAXX. One patient with platinum- and PARP inhibitor-resistant BRCA wild-type ovarian cancer achieved an unconfirmed RECIST v1.1 partial response.
Conclusions: Tuvusertib demonstrated manageable safety and exposure-related target engagement. Further clinical evaluation of tuvusertib is ongoing.
©2024 The Authors; Published by the American Association for Cancer Research.
Figures



References
-
- Carrassa L, Damia G. DNA-damage response inhibitors: mechanisms and potential applications in cancer therapy. Cancer Treat Rev 2017;60:139–51. - PubMed
-
- Kantidze OL, Velichko AK, Luzhin AV, Petrova NV, Razin SV. Synthetically lethal interactions of ATM, ATR, and DNA-PKcs. Trends Cancer 2018;4:755–68. - PubMed
-
- Blackford AN, Jackson SP. ATM, ATR, and DNA-PK: the trinity at the heart of the DNA-damage response. Mol Cell 2017;66:801–17. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
