

COVID-19-Associated Acute Kidney Injury and Longitudinal Kidney Outcomes
- PMID: 38407862
- PMCID: PMC10897825
- DOI: 10.1001/jamainternmed.2023.8225
COVID-19-Associated Acute Kidney Injury and Longitudinal Kidney Outcomes
Abstract
Importance: COVID-19 infection is associated with a high incidence of acute kidney injury (AKI). Although rapid kidney function decline has been reported in the first few months after COVID-19-associated AKI (COVID-AKI), the longer-term association of COVID-AKI with kidney function remains unknown.
Objective: To assess long-term kidney outcomes of patients who had COVID-19-associated AKI.
Design, setting, and participants: This was a retrospective longitudinal multicenter cohort study conducted in a large hospital system using electronic health records data on adult hospitalized patients with AKI and COVID-19 or other illnesses. Included patients were hospitalized during the COVID-19 pandemic (March 2020-June 2022), were screened for SARS-CoV-2, had AKI, and survived to discharge, or had been hospitalized during the 5 years before the pandemic (October 2016-January 2020), had a positive influenza A or B test result, had AKI, and survived to discharge. Patients were followed up for a maximum of 2 years after hospital discharge. Data analyses were performed from December 2022 to November 2023.
Exposure: COVID-19 and influenza.
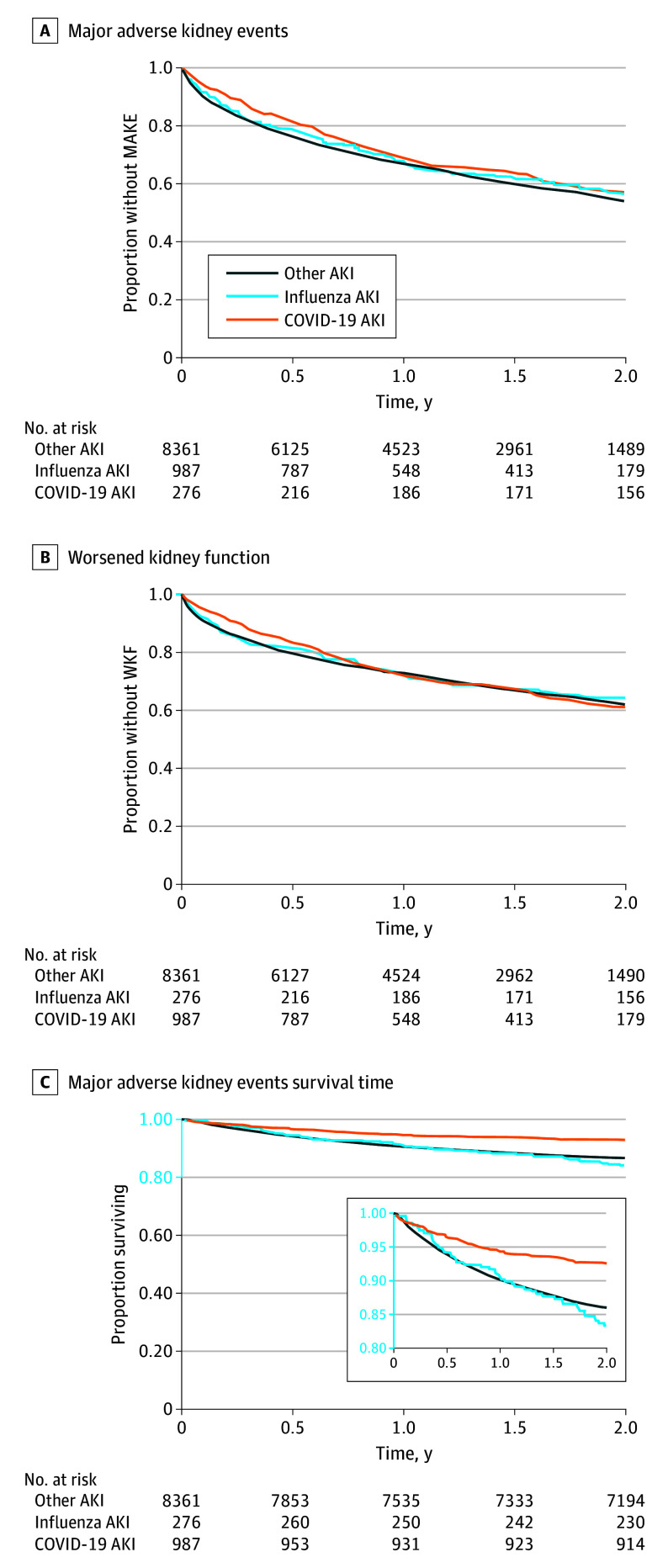
Main outcomes and measures: The primary outcome was major adverse kidney events (MAKE), defined as a composite of mortality and worsened kidney function (estimated glomerular filtration rate [eGFR] decline by ≥25% from discharge eGFR or kidney failure requiring dialysis). Multivariable time-to-event analyses were performed to compare MAKE between individuals with COVID-AKI and those who had AKI associated with other illnesses hospitalized during the same period. For further comparison, this outcome was assessed for a historic cohort of patients with influenza-associated AKI.
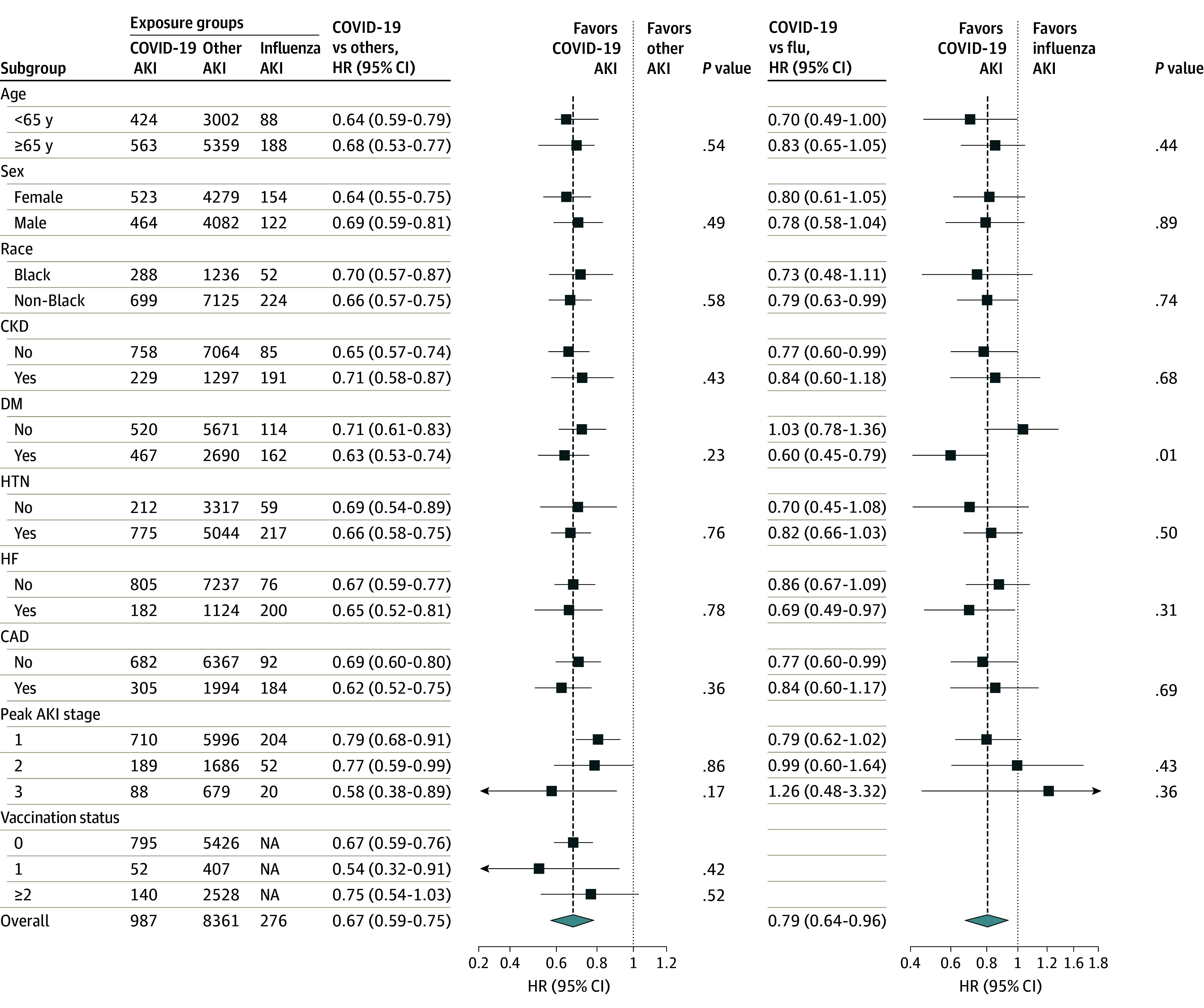
Results: The study cohort included 9624 hospitalized patients (mean [SD] age, 69.0 [15.7] years; 4955 [51.5%] females) with AKI, including 987 patients with COVID-AKI, 276 with influenza-associated AKI, and 8361 with AKI associated with other illnesses (other-AKI). Compared with the other 2 groups, patients with COVID-19-associated AKI were slightly younger in age, had a higher baseline eGFR, worse baseline comorbidity scores, higher markers of illness severity, and longer hospital stay. Compared with the other-AKI group, the COVID-AKI group had lower MAKE (adjusted hazard ratio [aHR], 0.67; 95% CI, 0.59-0.75) due to lower all-cause mortality (aHR, 0.31; 95% CI, 0.24-0.39) and lower rates of worsened kidney function (aHR, 0.78; 95% CI, 0.69-0.88).
Conclusions and relevance: The findings of this multicenter cohort study indicate that survivors of hospitalization with COVID-AKI experience lower rates of MAKE, long-term kidney function decline, and mortality compared with patients with AKI associated with other illnesses.
Conflict of interest statement
Figures
Similar articles
-
Assessment of Acute Kidney Injury and Longitudinal Kidney Function After Hospital Discharge Among Patients With and Without COVID-19.JAMA Netw Open. 2021 Mar 1;4(3):e211095. doi: 10.1001/jamanetworkopen.2021.1095. JAMA Netw Open. 2021. PMID: 33688965 Free PMC article.
-
Outcomes Among Patients Hospitalized With COVID-19 and Acute Kidney Injury.Am J Kidney Dis. 2021 Feb;77(2):204-215.e1. doi: 10.1053/j.ajkd.2020.09.002. Epub 2020 Sep 19. Am J Kidney Dis. 2021. PMID: 32961245 Free PMC article.
-
Kidney Recovery and Death in Critically Ill Patients With COVID-19-Associated Acute Kidney Injury Treated With Dialysis: The STOP-COVID Cohort Study.Am J Kidney Dis. 2022 Mar;79(3):404-416.e1. doi: 10.1053/j.ajkd.2021.11.004. Epub 2021 Dec 4. Am J Kidney Dis. 2022. PMID: 34871701 Free PMC article.
-
Study of Incidence, Clinical profile and Outcomes among patients hospitalized for COVID-19 with Acute Kidney Injury.J Assoc Physicians India. 2022 Apr;70(4):11-12. J Assoc Physicians India. 2022. PMID: 35443445 Review.
-
Are Kidneys Affected by SARS-CoV-2 Infection? An Updated Review on COVID-19-Associated AKI.Pathogens. 2024 Apr 16;13(4):325. doi: 10.3390/pathogens13040325. Pathogens. 2024. PMID: 38668280 Free PMC article. Review.
Cited by
-
Classification and Regression Trees analysis identifies patients at high risk for kidney function decline following hospitalization.PLoS One. 2025 Jan 31;20(1):e0317558. doi: 10.1371/journal.pone.0317558. eCollection 2025. PLoS One. 2025. PMID: 39888928 Free PMC article.
-
Incidence of major adverse kidney events after ICU admission in COVID-19 and non-COVID-19 ARDS patients.BMJ Open. 2025 May 6;15(5):e094887. doi: 10.1136/bmjopen-2024-094887. BMJ Open. 2025. PMID: 40328653 Free PMC article.
-
SARS-CoV-2 Spike Protein Amplifies the Immunogenicity of Healthy Renal Epithelium in the Presence of Renal Cell Carcinoma.Cells. 2024 Dec 10;13(24):2038. doi: 10.3390/cells13242038. Cells. 2024. PMID: 39768130 Free PMC article.
-
COVID-19 and Diabetes: Persistent Cardiovascular and Renal Risks in the Post-Pandemic Landscape.Life (Basel). 2025 Apr 30;15(5):726. doi: 10.3390/life15050726. Life (Basel). 2025. PMID: 40430154 Free PMC article. Review.
-
Integrated Transcriptomic Analysis Reveals Reciprocal Interactions between SARS-CoV-2 Infection and Multi-Organ Dysfunction, Especially the Correlation of Renal Failure and COVID-19.Life (Basel). 2024 Jul 30;14(8):960. doi: 10.3390/life14080960. Life (Basel). 2024. PMID: 39202702 Free PMC article.
References
-
- Nadim MK, Forni LG, Mehta RL, et al. . COVID-19-associated acute kidney injury: consensus report of the 25th Acute Disease Quality Initiative (ADQI) Workgroup [published correction appears in Nat Rev Nephrol. 2020 Nov 2]. Nat Rev Nephrol. 2020;16(12):747-764. doi:10.1038/s41581-020-00356-5 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
