

Functional Outcomes in Conservatively vs Surgically Treated Cerebellar Infarcts
- PMID: 38407889
- PMCID: PMC10897822
- DOI: 10.1001/jamaneurol.2023.5773
Functional Outcomes in Conservatively vs Surgically Treated Cerebellar Infarcts
Abstract
Importance: According to the current American Heart Association/American Stroke Association guidelines, decompressive surgery is indicated in patients with cerebellar infarcts that demonstrate severe cerebellar swelling. However, there is no universal definition of swelling and/or infarct volume(s) available to support a decision for surgery.
Objective: To evaluate functional outcomes in surgically compared with conservatively managed patients with cerebellar infarcts.
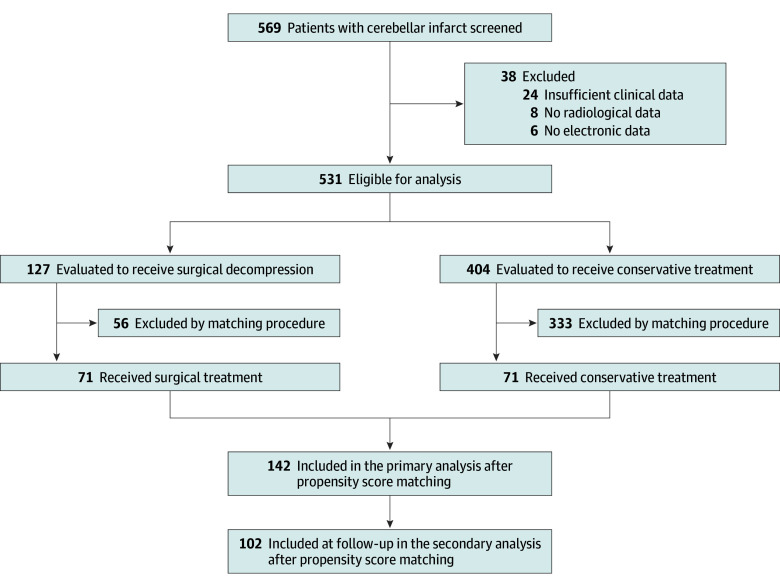
Design, setting, and participants: In this retrospective multicenter cohort study, patients with cerebellar infarcts treated at 5 tertiary referral hospitals or stroke centers within Germany between 2008 and 2021 were included. Data were analyzed from November 2020 to November 2023.
Exposures: Surgical treatment (ie, posterior fossa decompression plus standard of care) vs conservative management (ie, medical standard of care).
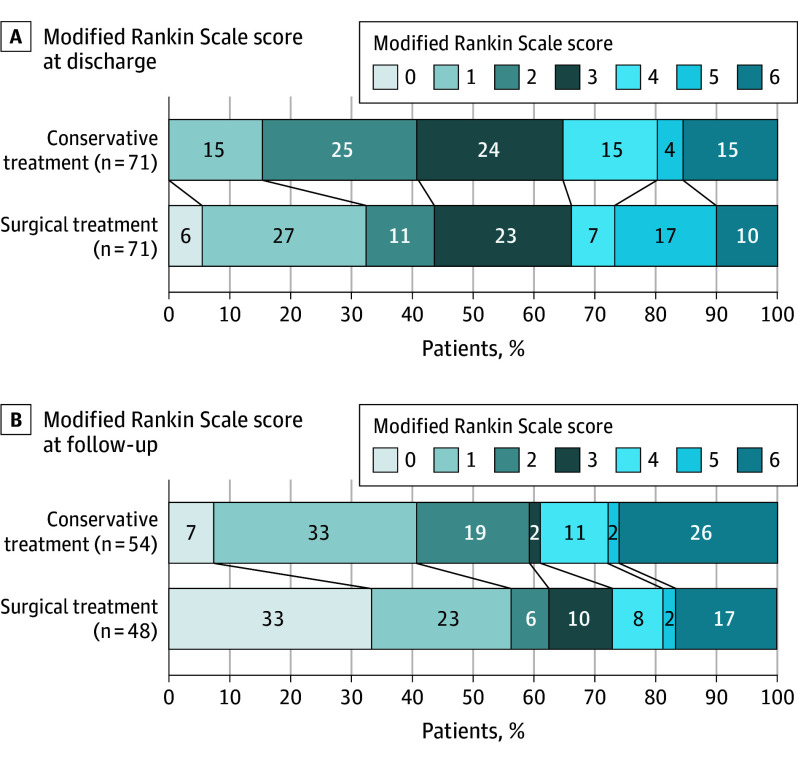
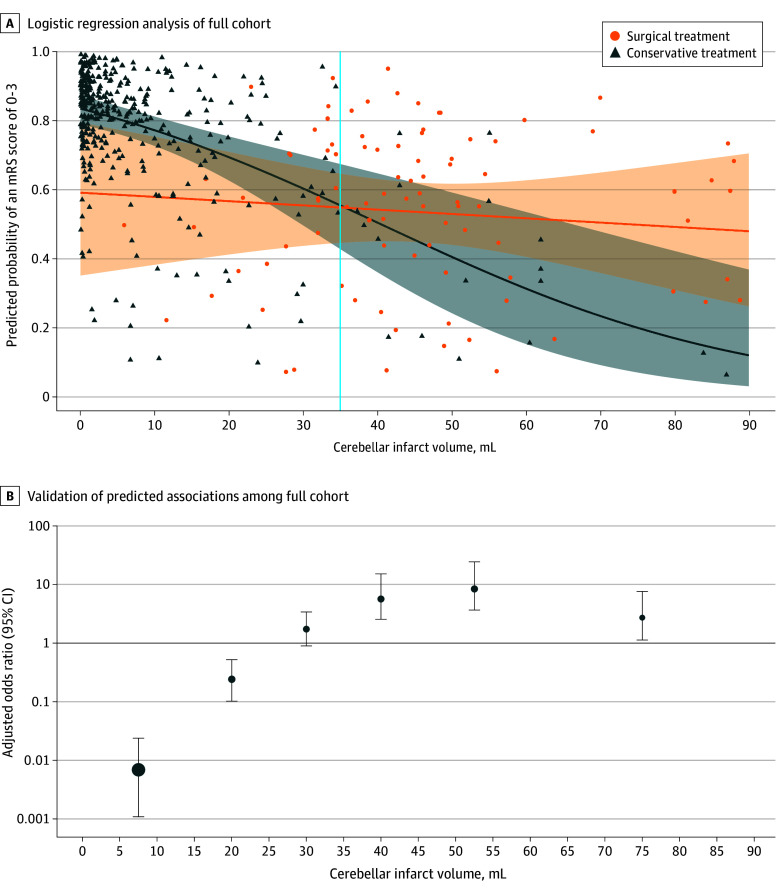
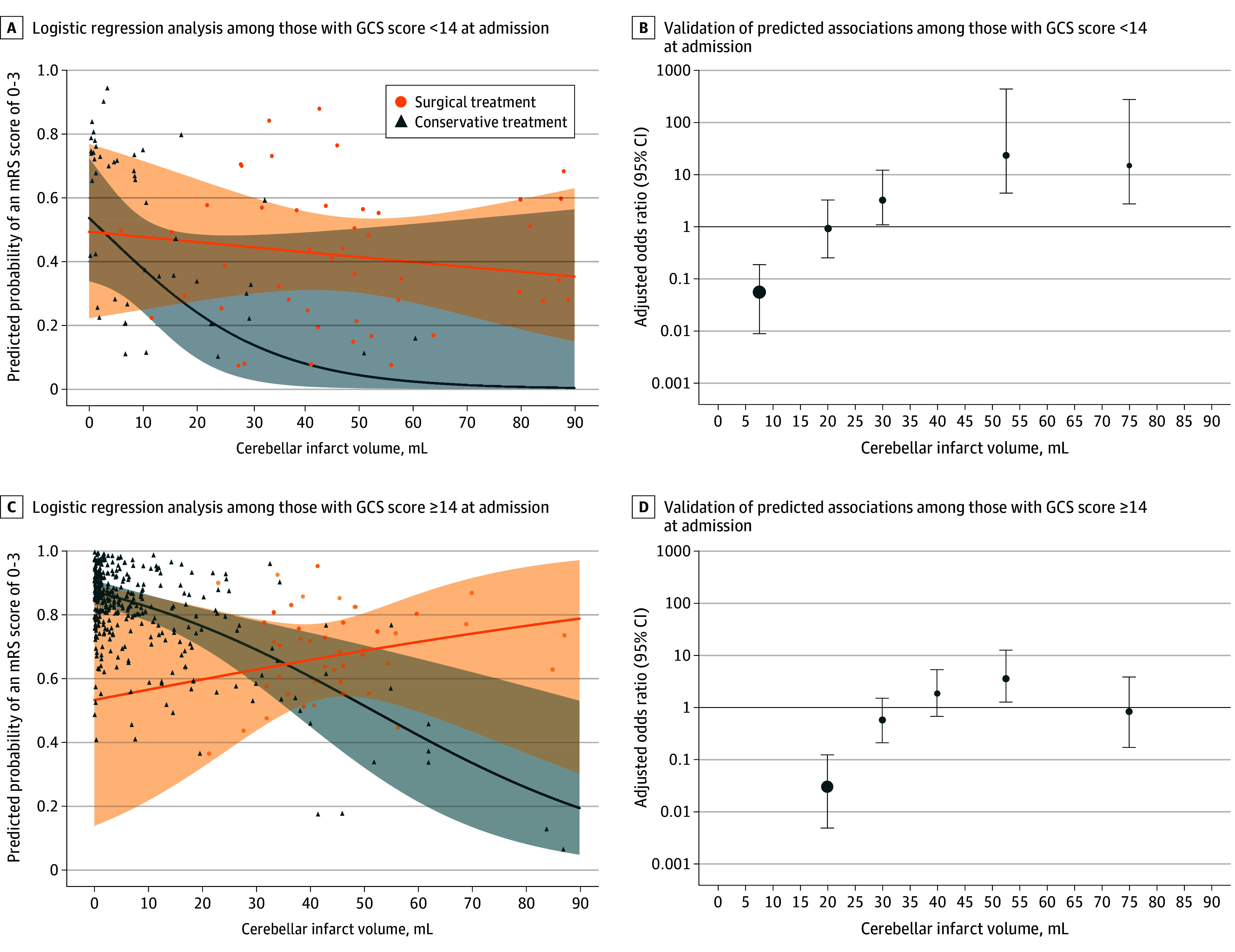
Main outcomes and measures: The primary outcome examined was functional status evaluated by the modified Rankin Scale (mRS) at discharge and 1-year follow-up. Secondary outcomes included the predicted probabilities for favorable outcome (mRS score of 0 to 3) stratified by infarct volumes or Glasgow Coma Scale score at admission and treatment modality. Analyses included propensity score matching, with adjustments for age, sex, Glasgow Coma Scale score at admission, brainstem involvement, and infarct volume.
Results: Of 531 included patients with cerebellar infarcts, 301 (57%) were male, and the mean (SD) age was 68 (14.4) years. After propensity score matching, a total of 71 patients received surgical treatment and 71 patients conservative treatment. There was no significant difference in favorable outcomes (ie, mRS score of 0 to 3) at discharge for those treated surgically vs conservatively (47 [66%] vs 45 [65%]; odds ratio, 1.1; 95% CI, 0.5-2.2; P > .99) or at follow-up (35 [73%] vs 33 [61%]; odds ratio, 1.8; 95% CI, 0.7-4.2; P > .99). In patients with cerebellar infarct volumes of 35 mL or greater, surgical treatment was associated with a significant improvement in favorable outcomes at 1-year follow-up (38 [61%] vs 3 [25%]; odds ratio, 4.8; 95% CI, 1.2-19.3; P = .03), while conservative treatment was associated with favorable outcomes at 1-year follow-up in patients with infarct volumes of less than 25 mL (2 [34%] vs 218 [74%]; odds ratio, 0.2; 95% CI, 0-1.0; P = .047).
Conclusions and relevance: Overall, surgery was not associated with improved outcomes compared with conservative management in patients with cerebellar infarcts. However, when stratifying based on infarct volume, surgical treatment appeared to be beneficial in patients with larger infarct volumes, while conservative management appeared favorable in patients with smaller infarct volumes.
Conflict of interest statement
Figures
References
-
- Feigin VL, Stark BA, Johnson CO, et al. ; GBD 2019 Stroke Collaborators . Global, regional, and national burden of stroke and its risk factors, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021;20(10):795-820. doi:10.1016/S1474-4422(21)00252-0 - DOI - PMC - PubMed
-
- Hofmeijer J, Kappelle LJ, Algra A, Amelink GJ, van Gijn J, van der Worp HB; HAMLET Investigators . Surgical decompression for space-occupying cerebral infarction (the Hemicraniectomy After Middle Cerebral Artery infarction with Life-threatening Edema Trial [HAMLET]): a multicentre, open, randomised trial. Lancet Neurol. 2009;8(4):326-333. doi:10.1016/S1474-4422(09)70047-X - DOI - PubMed
LinkOut - more resources
Full Text Sources
