

RAS-Mutated Cytologically Indeterminate Thyroid Nodules: Prevalence of Malignancy and Behavior Under Active Surveillance
- PMID: 38407967
- PMCID: PMC11971614
- DOI: 10.1089/thy.2023.0544
RAS-Mutated Cytologically Indeterminate Thyroid Nodules: Prevalence of Malignancy and Behavior Under Active Surveillance
Abstract
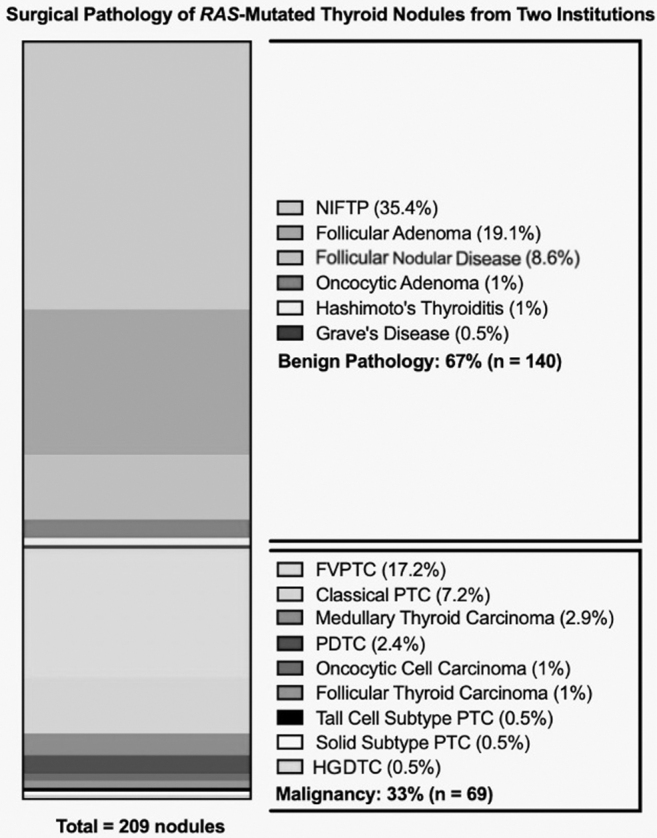
Background: Genomic profiling is now available for risk stratification of cytologically indeterminate thyroid nodules (ITNs). Mutations in RAS genes (HRAS, NRAS, KRAS) are found in both benign and malignant thyroid nodules, although isolated RAS mutations are rarely associated with aggressive tumors. Because the long-term behavior of RAS-mutant ITNs is not well understood, most undergo immediate surgery. In this multicenter retrospective cohort study, we characterize tumor growth kinetics of RAS-mutant ITNs followed with active surveillance (AS) using serial ultrasound (US) scans and examine the histopathologic diagnoses of those surgically resected. Methods: US and histopathologic data were analyzed retrospectively from two cohorts: (1) RAS-mutant ITNs managed with AS at three institutions (2010-2023) and (2) RAS-mutant ITNs managed with immediate surgery at two institutions (2016-2020). AS cohort subjects had ≥3 months of follow-up and two or more US scans. Cumulative incidence of nodule growth was determined by the Kaplan-Meier method and growth by ≥72% change in tumor volume. Pathological diagnoses for the immediate surgery cohort were analyzed separately. Results: Sixty-two patients with 63 RAS-mutated ITNs under AS had a median diameter of 1.7 cm (interquartile range [IQR] 1.2-2.6) at time of diagnosis. During a median AS period of 23 months (IQR 9.5-53.5 months), growth was observed in 12 of 63 nodules (19.0%), with a cumulative incidence of 1.9% (1 year), 23.0% (3 years), and 28.0% (5 years). Most nodules (81.0%) demonstrated stability. Surgery was ultimately performed in 6 nodules, of which 1 (16.7%) was malignant. In the cohort of 209 RAS-mutant ITNs triaged to immediate surgery, 33% were malignant (23.9% American Thyroid Association [ATA] low-risk cancers, 7.2% ATA intermediate-risk, and 1.9% ATA high-risk. During a median follow-up of 6.9 (IQR 4.4-7.1) years, there were no disease-specific deaths in these patients. Conclusions: We describe the behavior of RAS-mutant ITNs under AS and find that most demonstrate stability over time. Of the resected RAS-mutant nodules, most were benign; of the cancers, most were ATA low-risk. Immediate surgical resection of all RAS-mutant ITNs appears to be a low-value practice. Further research is needed to help define cases most appropriate for AS or immediate surgery.
Keywords: RAS gene mutation; ThyroSeq; active surveillance; cytologically indeterminate thyroid nodules; thyroid nodules.
Figures




References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
