

Quantitative PCR as a marker for preemptive therapy and its role in therapeutic control in Trypanosoma cruzi/HIV coinfection
- PMID: 38408095
- PMCID: PMC10896531
- DOI: 10.1371/journal.pntd.0011961
Quantitative PCR as a marker for preemptive therapy and its role in therapeutic control in Trypanosoma cruzi/HIV coinfection
Abstract
Background: Trypanosoma cruzi and HIV coinfection can evolve with depression of cellular immunity and increased parasitemia. We applied quantitative PCR (qPCR) as a marker for preemptive antiparasitic treatment to avoid fatal Chagas disease reactivation and analyzed the outcome of treated cases.
Methodology: This mixed cross-sectional and longitudinal study included 171 Chagas disease patients, 60 coinfected with HIV. Of these 60 patients, ten showed Chagas disease reactivation, confirmed by parasites identified in the blood, cerebrospinal fluid, or tissues, 12 exhibited high parasitemia without reactivation, and 38 had low parasitemia and no reactivation.
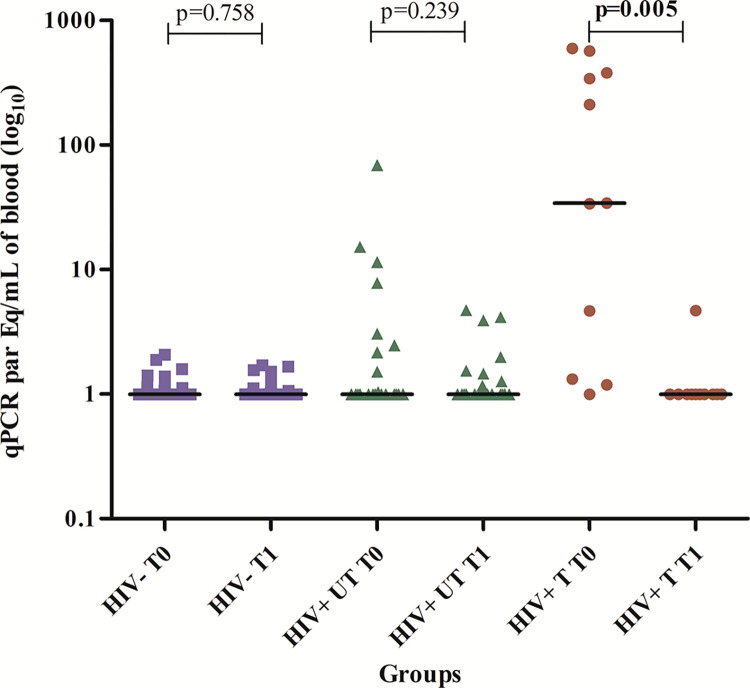
Results: We showed, for the first time, the success of the timely introduction of benznidazole in the non-reactivated group with high levels of parasitemia detected by qPCR and the absence of parasites in reactivated cases with at least 58 days of benznidazole. All HIV+ patients with or without reactivation had a 4.0-5.1 higher chance of having parasitemia than HIV seronegative cases. A positive correlation was found between parasites and viral loads. Remarkably, treated T. cruzi/HIV-coinfected patients had 77.3% conversion from positive to negative parasitemia compared to 19.1% of untreated patients. Additionally, untreated patients showed ~13.6 times higher Odds Ratio of having positive parasitemia in the follow-up period compared with treated patients. Treated and untreated patients showed no differences regarding the evolution of Chagas disease. The main factors associated with all-cause mortality were higher parasitemia, lower CD4 counts/μL, higher viral load, and absence of antiretroviral therapy.
Conclusion: We recommend qPCR prospective monitoring of T. cruzi parasitemia in HIV+ coinfected patients and point out the value of pre-emptive therapy for those with high parasitemia. In parallel, early antiretroviral therapy introduction is advisable, aiming at viral load control, immune response restoration, and increasing survival. We also suggest an early antiparasitic treatment for all coinfected patients, followed by effectiveness analysis alongside antiretroviral therapy.
Copyright: © 2024 de Freitas et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
I have read the journal’s policy and the authors of this manuscript have the following competing interests: CB is an expert paid consultant on ancestry and diversity for Roche/Genentech. The other authors have no competing interests.
Figures
Similar articles
-
Real-time PCR in HIV/Trypanosoma cruzi coinfection with and without Chagas disease reactivation: association with HIV viral load and CD4 level.PLoS Negl Trop Dis. 2011 Aug;5(8):e1277. doi: 10.1371/journal.pntd.0001277. Epub 2011 Aug 30. PLoS Negl Trop Dis. 2011. PMID: 21912712 Free PMC article.
-
HIV and Chagas Disease: An Evaluation of the Use of Real-Time Quantitative Polymerase Chain Reaction to Measure Levels of Trypanosoma cruzi Parasitemia in HIV Patients in Cochabamba, Bolivia.Am J Trop Med Hyg. 2021 Aug 16;105(3):643-650. doi: 10.4269/ajtmh.20-1141. Am J Trop Med Hyg. 2021. PMID: 34398818 Free PMC article.
-
Use of a Chagas Urine Nanoparticle Test (Chunap) to Correlate with Parasitemia Levels in T. cruzi/HIV Co-infected Patients.PLoS Negl Trop Dis. 2016 Feb 26;10(2):e0004407. doi: 10.1371/journal.pntd.0004407. eCollection 2016 Feb. PLoS Negl Trop Dis. 2016. PMID: 26919324 Free PMC article.
-
Immunosuppression and Chagas disease: a management challenge.PLoS Negl Trop Dis. 2013;7(1):e1965. doi: 10.1371/journal.pntd.0001965. Epub 2013 Jan 17. PLoS Negl Trop Dis. 2013. PMID: 23349998 Free PMC article. Review.
-
Trypanocidal drugs for late-stage, symptomatic Chagas disease (Trypanosoma cruzi infection).Cochrane Database Syst Rev. 2020 Dec 11;12(12):CD004102. doi: 10.1002/14651858.CD004102.pub3. Cochrane Database Syst Rev. 2020. PMID: 33305846 Free PMC article.
Cited by
-
Quantitative PCR for parasitemia monitoring and preemptive therapy in patients with Chagas disease and autoimmune rheumatic disorders undergoing biologic treatment: a case series.Rev Soc Bras Med Trop. 2025 Jun 2;58:e008022025. doi: 10.1590/0037-8682-0419-2024. eCollection 2025. Rev Soc Bras Med Trop. 2025. PMID: 40465888 Free PMC article.
-
From Tradition to Innovation: Diverse Molecular Techniques in the Fight Against Infectious Diseases.Diagnostics (Basel). 2024 Dec 21;14(24):2876. doi: 10.3390/diagnostics14242876. Diagnostics (Basel). 2024. PMID: 39767237 Free PMC article. Review.
References
-
- World Health Organization. Chagas disease (also known as American trypanosomiasis) 01/04/2021 (cited 2022 January 12) Available from: https://www.who.int/news-room/fact-sheets/detail/chagas-disease-(america....
-
- Virreira M, Truyens C, Alonso-Vega C, Brutus L, Jijena J, Torrico F, et al.. Comparison of Trypanosoma cruzi and lineages and levels of parasitic DNA infected mothers and their newborns. Am J Trop Med Hyg. 2007; 77: 102–106 - PubMed
-
- Angheben A, Anselmi M, Gobbi F, Marocco S, Monteiro G, Buonfrate D, et al.. Chagas disease in Italy: breaking an epidemiological silence. Euro Surveill. 2011;16(37):19969. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
