

Implementation strategies to build mental health-care capacity in Malawi: a health-economic evaluation
- PMID: 38408461
- PMCID: PMC10958395
- DOI: 10.1016/S2214-109X(23)00597-1
Implementation strategies to build mental health-care capacity in Malawi: a health-economic evaluation
Abstract
Background: Depression is a major contributor to morbidity and mortality in sub-Saharan Africa. Due to low system capacity, three in four patients with depression in sub-Saharan Africa go untreated. Despite this, little attention has been paid to the cost-effectiveness of implementation strategies to scale up evidence-based depression treatment in the region. In this study, we investigate the cost-effectiveness of two different implementation strategies to integrate the Friendship Bench approach and measurement-based care in non-communicable disease clinics in Malawi.
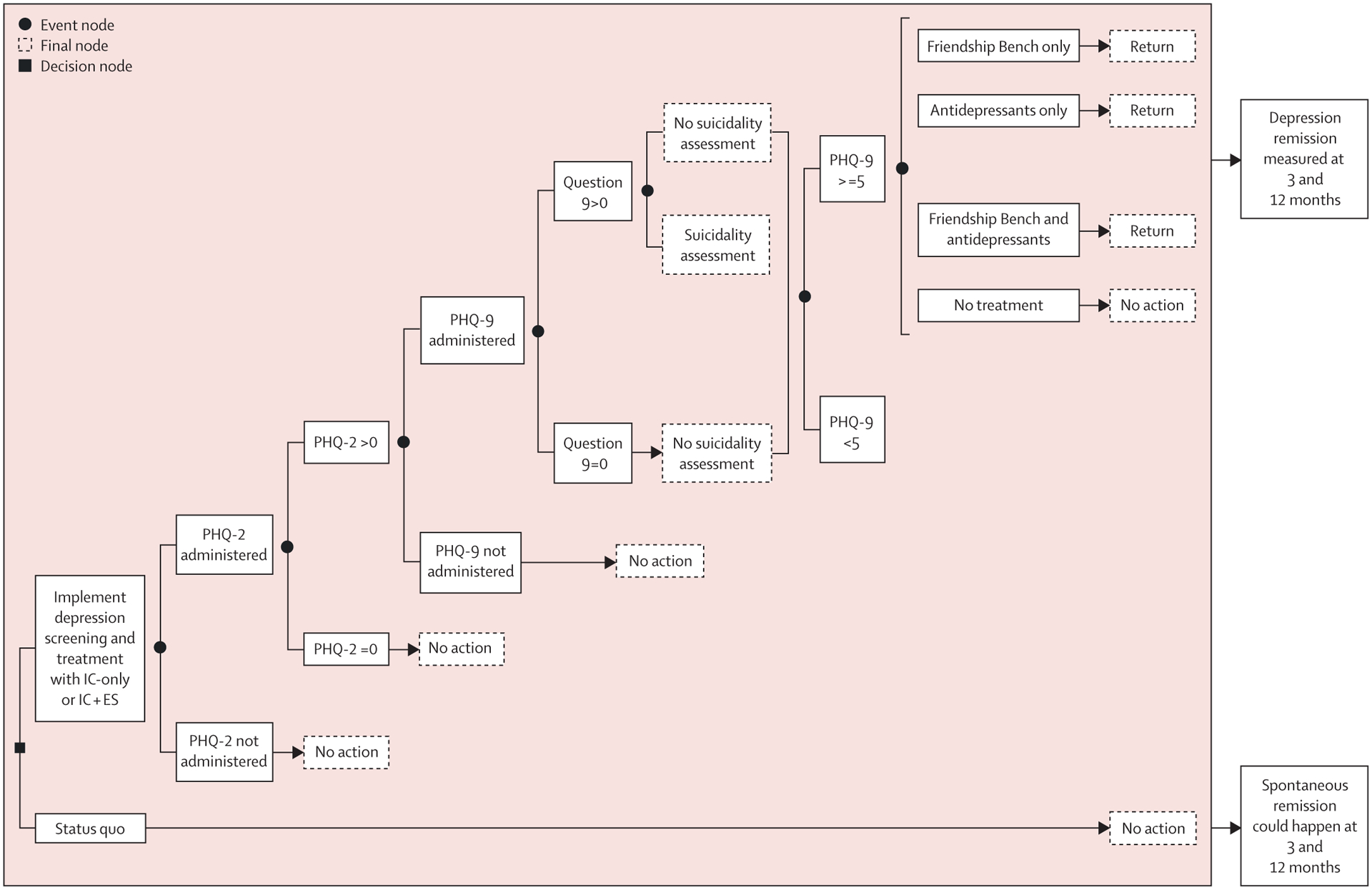
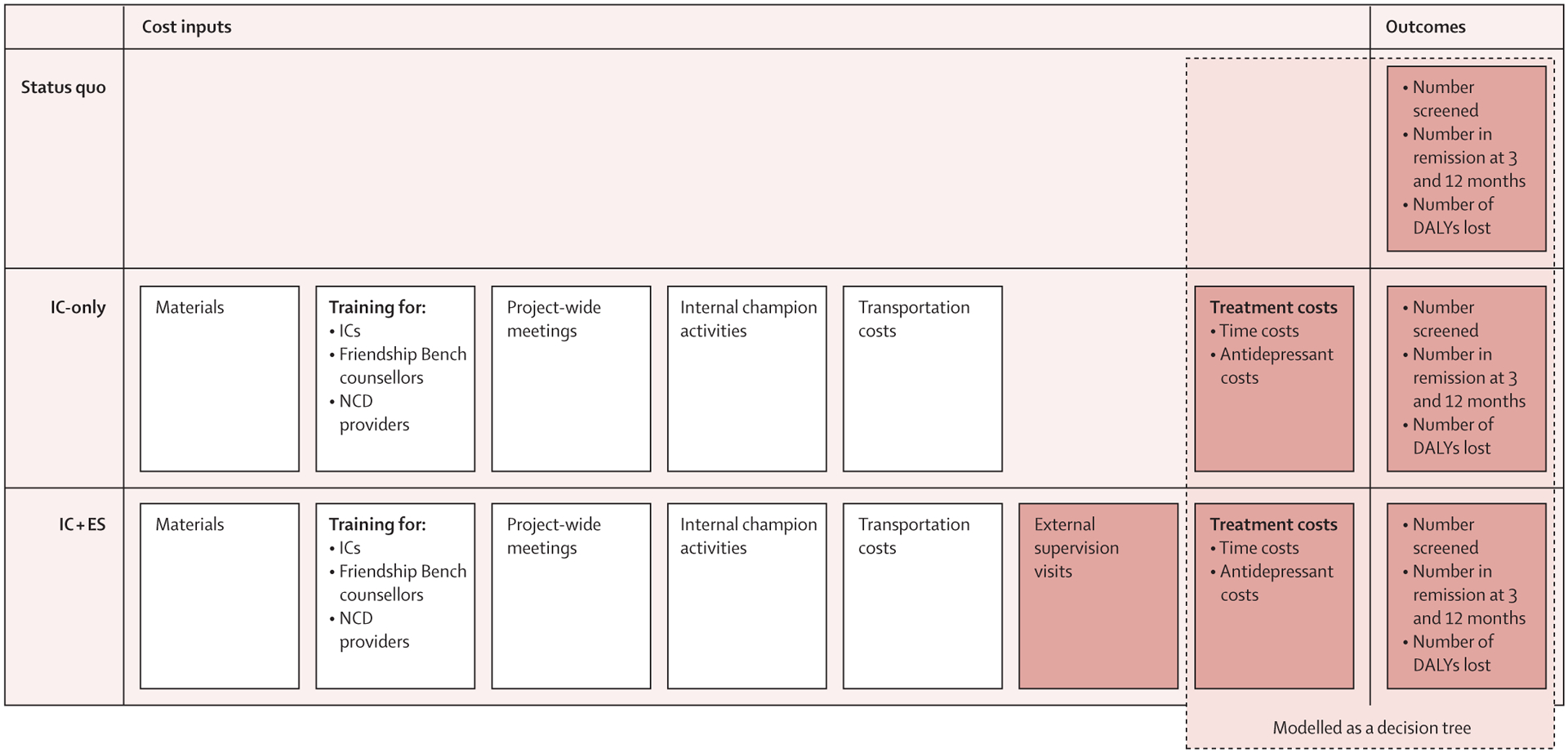
Methods: The two implementation strategies tested in this study are part of a trial, in which ten clinics were randomly assigned (1:1) to a basic implementation package consisting of an internal coordinator acting as a champion (IC-only group) or to an enhanced package that complemented the basic package with quarterly external supervision, and audit and feedback of intervention delivery (IC + ES group). We included material costs, training costs, costs related to project-wide meetings, transportation and medication costs, time costs related to internal champion activities and depression screening or treatment, and costs of external supervision visits if applicable. Outcomes included the number of patients screened with the patient health questionnaire 2 (PHQ-2), cases of remitted depression at 3 and 12 months, and disability-adjusted life-years (DALYs) averted. We compared the cost-effectiveness of both packages to the status quo (ie, no intervention) using a micro-costing-informed decision-tree model.
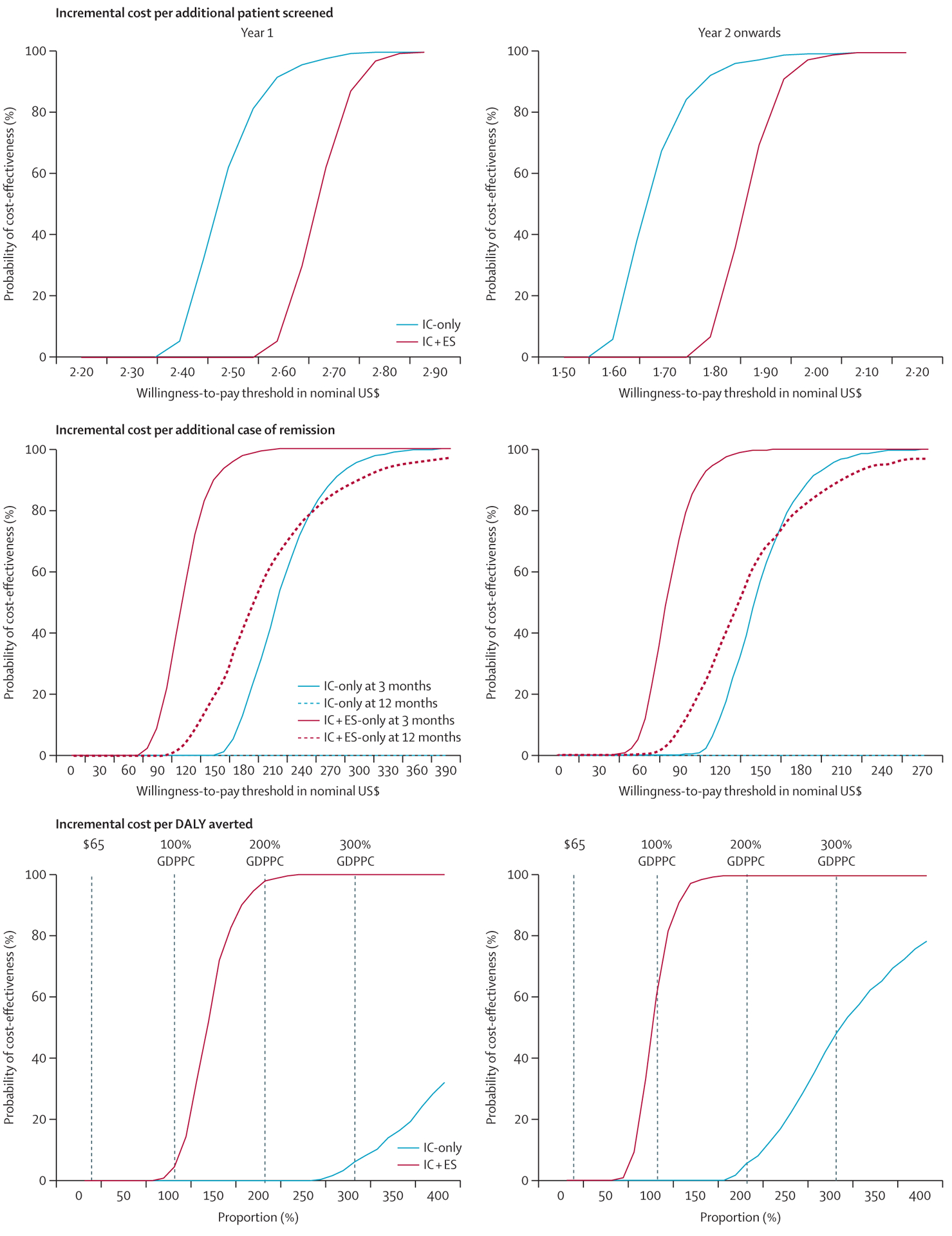
Findings: Relative to the status quo, IC + ES would be on average US$10 387 ($1349-$17 365) more expensive than IC-only but more effective in achieving remission and averting DALYs. The cost per additional remission would also be lower with IC + ES than IC-only at 3 months ($119 vs $223) and 12 months ($210 for IC + ES; IC-only dominated by the status quo at 12 months). Neither package would be cost-effective under the willingness-to-pay threshold of $65 per DALY averted currently used by the Malawian Ministry of Health. However, the IC + ES package would be cost-effective in relation to the commonly used threshold of three times per-capita gross domestic product per DALY averted.
Interpretation: Investing in supporting champions might be an appropriate use of resources. Although not currently cost-effective by Malawian willingness-to-pay standards compared with the status quo, the IC + ES package would probably be a cost-effective way to build mental health-care capacity in resource-constrained settings in which decision makers use higher willingness-to-pay thresholds.
Funding: National Institute of Mental Health.
Copyright © 2024 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY-NC-ND 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests BWP and BNG received grant funding for this work from the National Institute of Mental Health (paid to their institution). BWP also received support from the National Institutes of Health to attend meetings or travel for projects, or both, unrelated to this work. MCH received grant funding from the National Institute of Health (paid to their institution), for the submitted manuscript. SBW receives grant funding from Pfizer and AstraZeneca (paid to their institution), outside the submitted work. All other authors declare no competing interests.
Figures
Comment in
-
Cost-effectiveness of task-shifting in resource-constrained settings.Lancet Glob Health. 2024 Apr;12(4):e546-e547. doi: 10.1016/S2214-109X(24)00038-X. Epub 2024 Feb 23. Lancet Glob Health. 2024. PMID: 38408463 No abstract available.
Similar articles
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of paclitaxel, docetaxel, gemcitabine and vinorelbine in non-small-cell lung cancer.Health Technol Assess. 2001;5(32):1-195. doi: 10.3310/hta5320. Health Technol Assess. 2001. PMID: 12065068
-
The effectiveness and cost-effectiveness of carmustine implants and temozolomide for the treatment of newly diagnosed high-grade glioma: a systematic review and economic evaluation.Health Technol Assess. 2007 Nov;11(45):iii-iv, ix-221. doi: 10.3310/hta11450. Health Technol Assess. 2007. PMID: 17999840
-
Adefovir dipivoxil and pegylated interferon alfa-2a for the treatment of chronic hepatitis B: a systematic review and economic evaluation.Health Technol Assess. 2006 Aug;10(28):iii-iv, xi-xiv, 1-183. doi: 10.3310/hta10280. Health Technol Assess. 2006. PMID: 16904047
-
Intravenous magnesium sulphate and sotalol for prevention of atrial fibrillation after coronary artery bypass surgery: a systematic review and economic evaluation.Health Technol Assess. 2008 Jun;12(28):iii-iv, ix-95. doi: 10.3310/hta12280. Health Technol Assess. 2008. PMID: 18547499
-
Comparison of Two Modern Survival Prediction Tools, SORG-MLA and METSSS, in Patients With Symptomatic Long-bone Metastases Who Underwent Local Treatment With Surgery Followed by Radiotherapy and With Radiotherapy Alone.Clin Orthop Relat Res. 2024 Dec 1;482(12):2193-2208. doi: 10.1097/CORR.0000000000003185. Epub 2024 Jul 23. Clin Orthop Relat Res. 2024. PMID: 39051924
Cited by
-
Can the digital economy foster advancements in the healthcare sector? - a case study using interprovincial data from China.BMC Public Health. 2025 Jan 17;25(1):196. doi: 10.1186/s12889-025-21372-9. BMC Public Health. 2025. PMID: 39825273 Free PMC article.
-
Barriers and potential solutions for effective integration of depression care into non-communicable diseases clinics in Malawi: a qualitative end-point evaluation of the SHARP randomized controlled trial.Int J Ment Health Syst. 2025 Mar 6;19(1):8. doi: 10.1186/s13033-025-00663-z. Int J Ment Health Syst. 2025. PMID: 40050899 Free PMC article.
-
Two implementation strategies to support the integration of depression screening and treatment into hypertension and diabetes care in Malawi (SHARP): parallel, cluster-randomised, controlled, implementation trial.Lancet Glob Health. 2024 Apr;12(4):e652-e661. doi: 10.1016/S2214-109X(23)00592-2. Epub 2024 Feb 23. Lancet Glob Health. 2024. PMID: 38408462 Free PMC article. Clinical Trial.
References
-
- Patel V Mental health in low- and middle-income countries. Br Med Bull 2007; 81–82: 81–96. - PubMed
-
- WHO. Mental Health Atlas 2011. Jan 1, 2011. https://apps.who.int/iris/bitstream/handle/10665/44697/9799241564359_eng... (accessed Nov 29, 2023).
-
- WHO. mhGAP Mental Health Gap Action Programme: scaling up care for mental, neurological, and substance use disorders. Jan 1, 2008. https://www.who.int/publications/i/item/9789241596206 (accessed Jan 3, 2024). - PubMed
-
- Chibanda D, Weiss HA, Verhey R, et al. Effect of a primary care-based psychological intervention on symptoms of common mental disorders in Zimbabwe: a randomized clinical trial. JAMA 2016; 316: 2618–26. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
