

Effectiveness of preconception weight loss interventions on fertility in women: a systematic review and meta-analysis
- PMID: 38408693
- PMCID: PMC11384273
- DOI: 10.1016/j.fertnstert.2024.02.038
Effectiveness of preconception weight loss interventions on fertility in women: a systematic review and meta-analysis
Abstract
Importance: Weight loss before conception is recommended for women with overweight or obesity to improve fertility outcomes, but evidence supporting this recommendation is mixed.
Objective: To examine the effectiveness of weight loss interventions using lifestyle modification and/or medication in women with overweight or obesity on pregnancy, live birth, and miscarriage.
Data sources: An electronic search of MEDLINE, Embase, Cochrane Library, including Cochrane Database of Systematic Reviews and Cochrane Central Register of Controlled Trials, and Cumulative Index to Nursing and Allied Health Literature was conducted through July 6, 2022, via Wiley.
Study selection and synthesis: Randomized controlled trials examining weight loss interventions through lifestyle and/or medication in women with overweight or obesity planning pregnancy were included. Random-effects meta-analysis was conducted, reporting the risk ratio (RR) for each outcome. Subgroup analyses were conducted by intervention type, type of control group, fertility treatment, intervention length, and body mass index (BMI).
Main outcome(s): Clinical pregnancy, live birth, and miscarriage events.
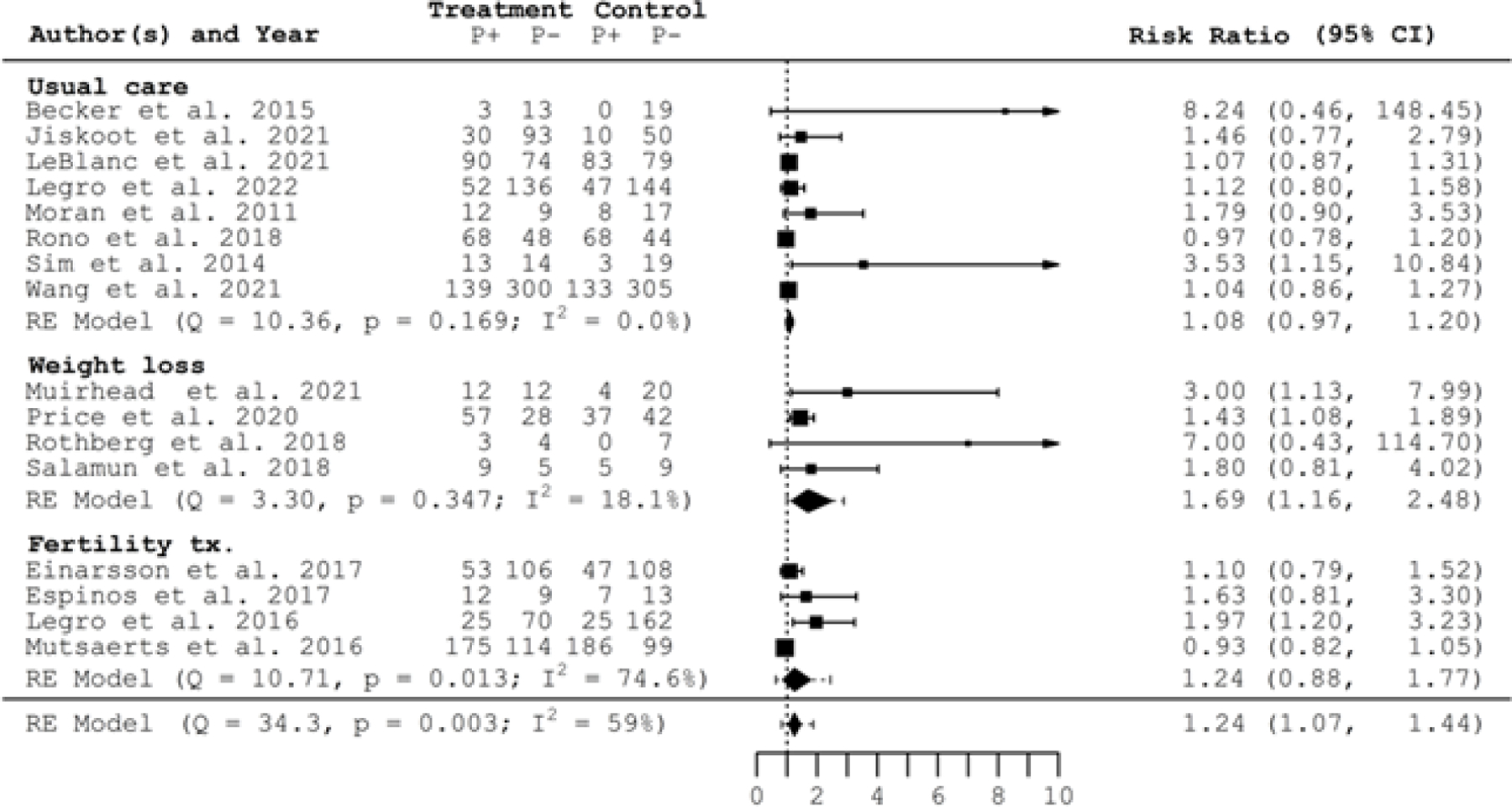
Result(s): A narrative review and meta-analysis were possible for 16 studies for pregnancy (n = 3,588), 13 for live birth (n = 3,329), and 11 for miscarriage (n = 3,248). Women randomized and exposed to a weight loss intervention were more likely to become pregnant (RR = 1.24, 95% CI 1.07-1.44; I2 = 59%) but not to have live birth (RR = 1.19, 95% CI 0.97-1.45; I2 = 69%) or miscarriage (RR = 1.17, 95% CI 0.79-1.74; I2 = 31%) compared with women in control groups. Subgroup analyses revealed women randomized to weight loss interventions lasting 12 weeks or fewer (n = 9, RR = 1.43; 95% CI 1.13-1.83) and women with a BMI ≥ 35 kg/m2 (n = 7, RR = 1.54; 95% CI, 1.18-2.02) were more likely to become pregnant compared with women in the control groups. Miscarriage was higher in intervention groups who underwent fertility treatment (n = 8, RR 1.45; 95% CI 1.07-1.96).
Conclusion(s): Pregnancy rates were higher in women undergoing preconception weight loss interventions with no impact on live birth or miscarriage rates. Findings do not support one-size-fits-all recommendation for weight loss through lifestyle modification and/or medication in women with overweight or obesity immediately before conception to improve live birth or miscarriage outcomes.
Keywords: Lifestyle intervention; antiobesity medication; overweight/obesity; preconception weight loss; pregnancy.
Copyright © 2024 American Society for Reproductive Medicine. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of Interests A.E.C. reports funding from K01 HL 143039 – Mentored Career Development Award from the NIH outside the submitted work. A.M.G. reports funding from NIH Grant P20GM144269 outside the submitted work. A.P.B. has nothing to disclose. J.M.N. has nothing to disclose. R.N.M. has nothing to disclose. H.S. has nothing to disclose. S.P. has nothing to disclose. T.N. has nothing to disclose. K.DS. has nothing to disclose. C.E. has nothing to disclose. N.S. has nothing to disclose.
Figures












References
-
- Mission JF, Marshall NE, Caughey AB. Pregnancy risks associated with obesity. Obstetrics and Gynecology Clinics 2015;42:335–53. - PubMed
-
- Talmor A, Dunphy B. Female obesity and infertility. Best practice & research Clinical obstetrics & gynaecology 2015;29:498–506. - PubMed
-
- McAuliffe FM, Killeen SL, Jacob CM, Hanson MA, Hadar E, McIntyre HD et al. Management of prepregnancy, pregnancy, and postpartum obesity from the FIGO Pregnancy and Non-Communicable Diseases Committee: A FIGO (International Federation of Gynecology and Obstetrics) guideline. International Journal of Gynaecology and Obstetrics 2020;151:16. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
