

Targeting HDAC6 to treat heart failure with preserved ejection fraction in mice
- PMID: 38409164
- PMCID: PMC10897156
- DOI: 10.1038/s41467-024-45440-7
Targeting HDAC6 to treat heart failure with preserved ejection fraction in mice
Erratum in
-
Author Correction: Targeting HDAC6 to treat heart failure with preserved ejection fraction in mice.Nat Commun. 2024 Oct 9;15(1):8749. doi: 10.1038/s41467-024-52831-3. Nat Commun. 2024. PMID: 39384783 Free PMC article. No abstract available.
Abstract
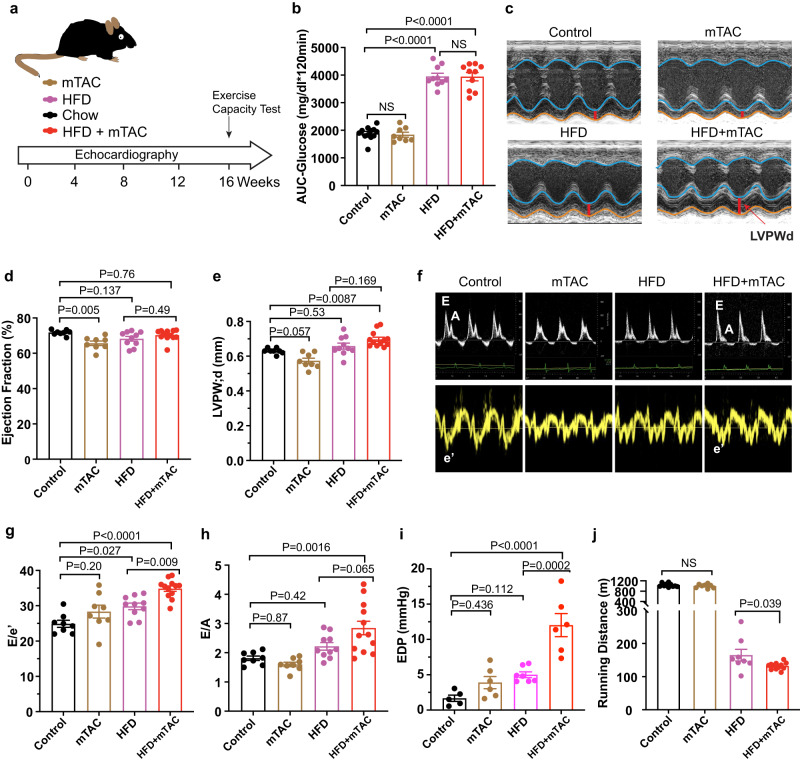
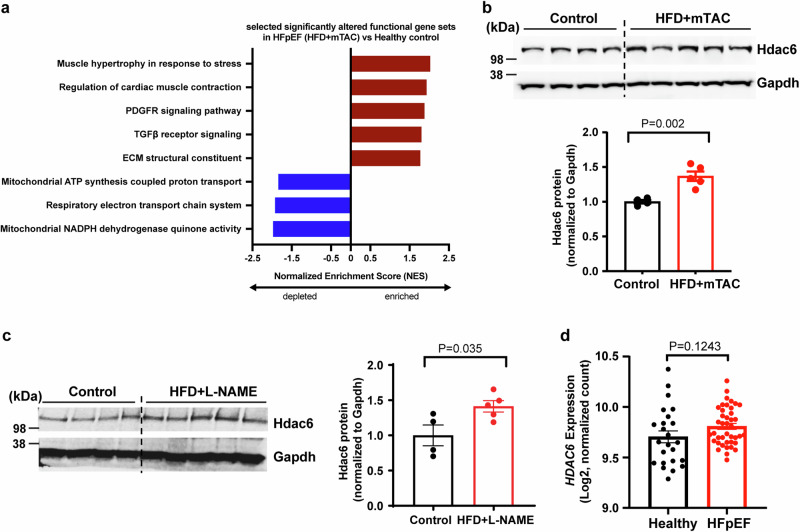
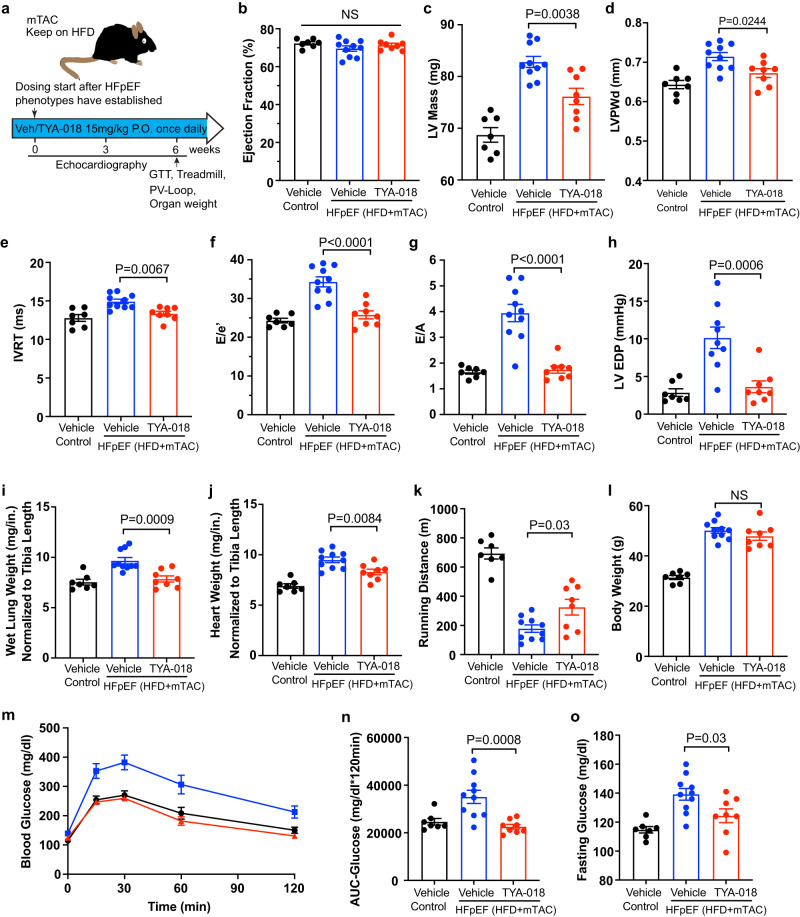
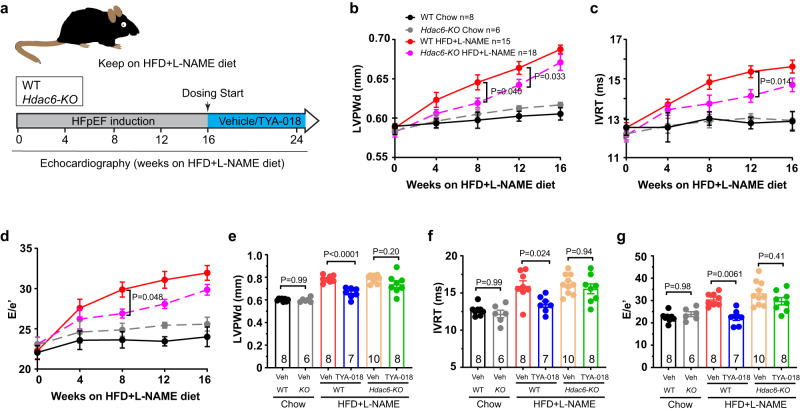
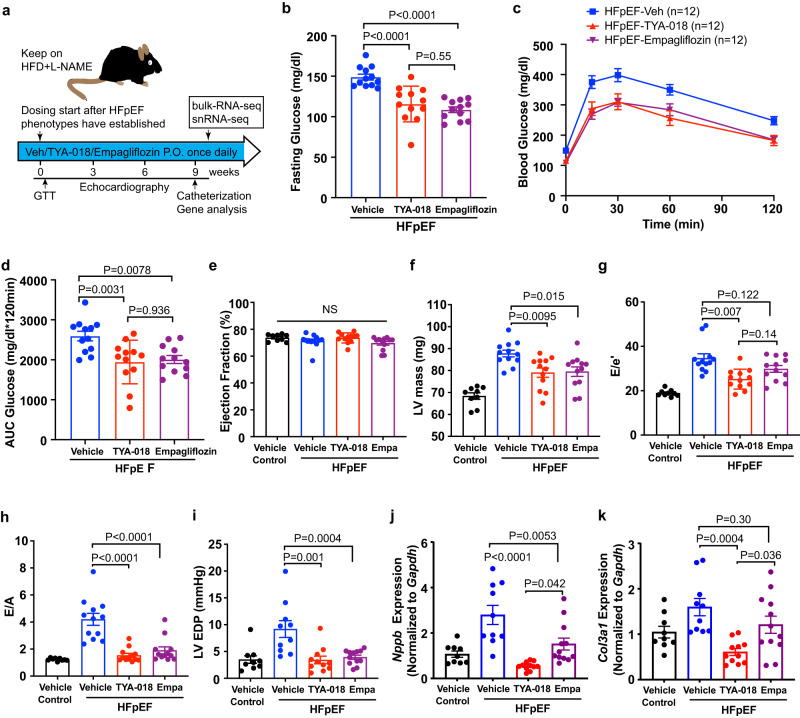
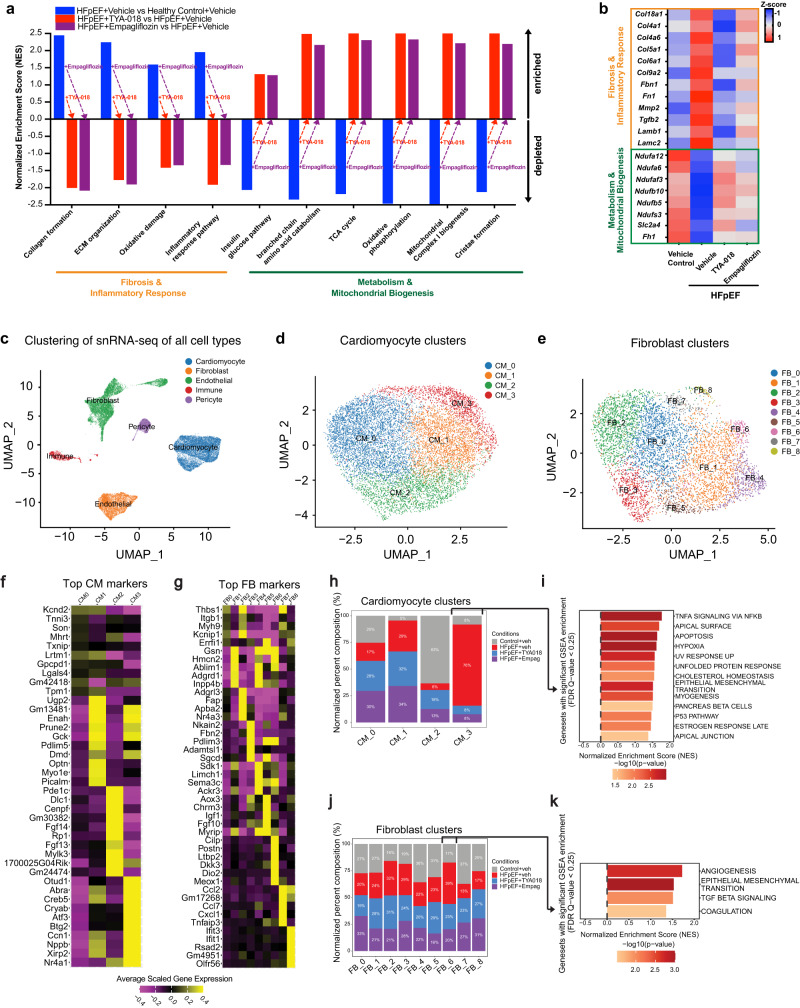
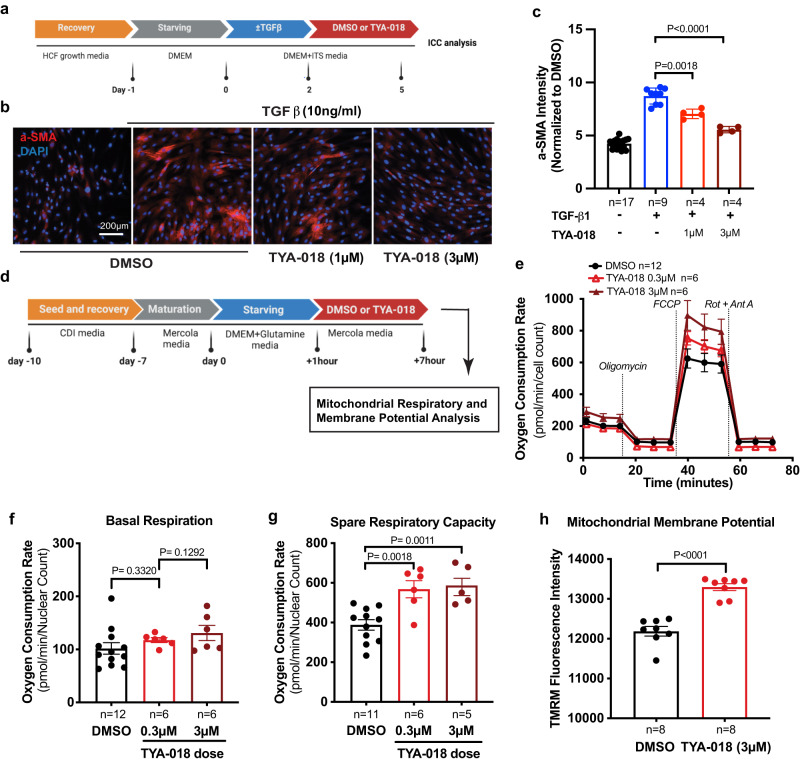
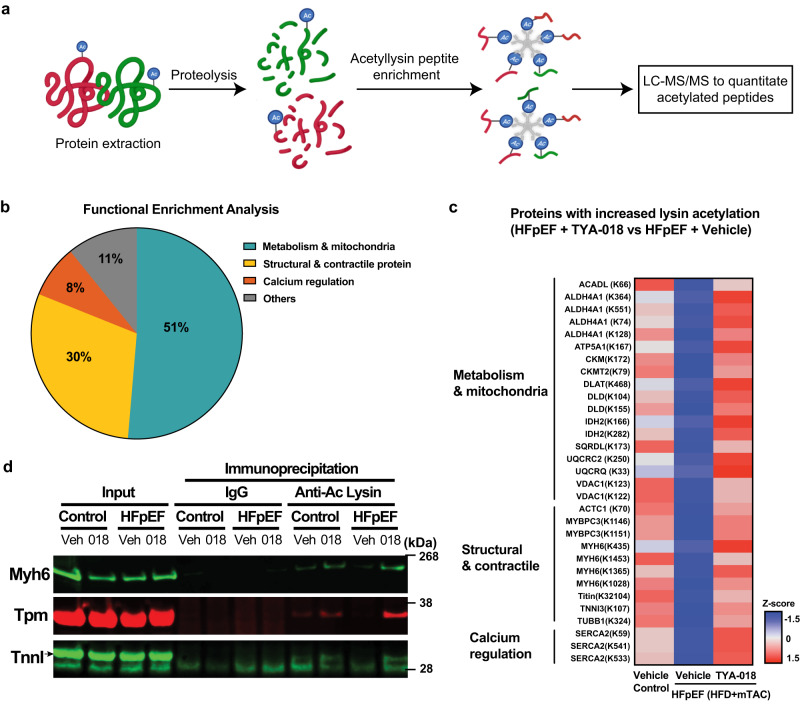
Heart failure with preserved ejection fraction (HFpEF) poses therapeutic challenges due to the limited treatment options. Building upon our previous research that demonstrates the efficacy of histone deacetylase 6 (HDAC6) inhibition in a genetic cardiomyopathy model, we investigate HDAC6's role in HFpEF due to their shared mechanisms of inflammation and metabolism. Here, we show that inhibiting HDAC6 with TYA-018 effectively reverses established heart failure and its associated symptoms in male HFpEF mouse models. Additionally, in male mice lacking Hdac6 gene, HFpEF progression is delayed and they are resistant to TYA-018's effects. The efficacy of TYA-018 is comparable to a sodium-glucose cotransporter 2 (SGLT2) inhibitor, and the combination shows enhanced effects. Mechanistically, TYA-018 restores gene expression related to hypertrophy, fibrosis, and mitochondrial energy production in HFpEF heart tissues. Furthermore, TYA-018 also inhibits activation of human cardiac fibroblasts and enhances mitochondrial respiratory capacity in cardiomyocytes. In this work, our findings show that HDAC6 impacts on heart pathophysiology and is a promising target for HFpEF treatment.
© 2024. The Author(s).
Conflict of interest statement
The authors of this publication are employed by Tenaya Therapeutics and hold stock in the company. This potential conflict of interest has been thoroughly reviewed and managed by Tenaya Therapeutics. There are no other competing interests.
Figures
References
-
- Heidenreich, P. A. et al. 2022 AHA/ACC/HFSA guideline for the management of heart failure: executive summary: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J. Am. Coll. Cardiol.79, 1757–1780 (2022). - PubMed
-
- Borlaug, B. A. Evaluation and management of heart failure with preserved ejection fraction. Nat. Rev. Cardiol.17, 559–573 (2020). - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
