

Optimal short-term outcomes in balloon pulmonary angioplasty: the minimum frequency of three sessions annually
- PMID: 38409856
- PMCID: PMC10898305
- DOI: 10.1177/17534666241232521
Optimal short-term outcomes in balloon pulmonary angioplasty: the minimum frequency of three sessions annually
Abstract
Background: Balloon pulmonary angioplasty (BPA) is typically performed in a sequential manner.
Objectives: This study aimed to determine the lowest frequency of BPA for patients who could not reach treatment goals in a short period.
Design: Retrospective cohort.
Methods: We retrospectively enrolled 186 BPA-treated patients diagnosed with chronic thromboembolic pulmonary hypertension. According to the accumulative number of performed BPA sessions or treated pulmonary vessels or the ratio of the number of treated pulmonary vessels/the number of baseline lesions (T/P) prior to the initial occurrence of clinical outcome or censored date, we divided patients into different groups. The principal outcome was clinical worsening.
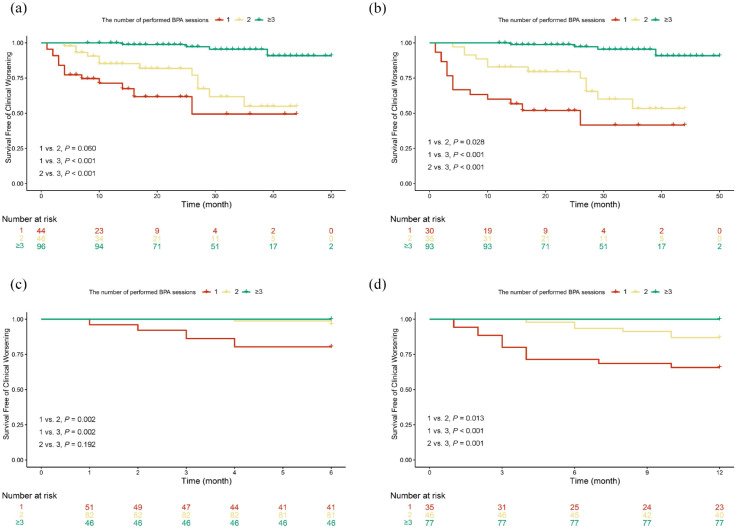
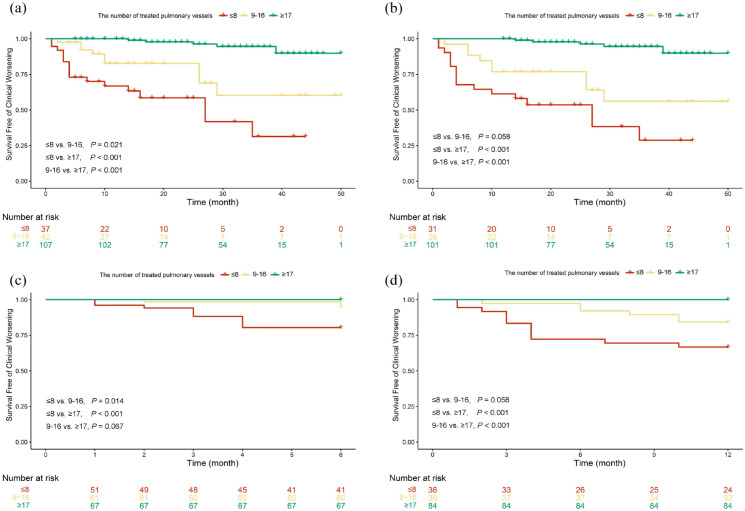
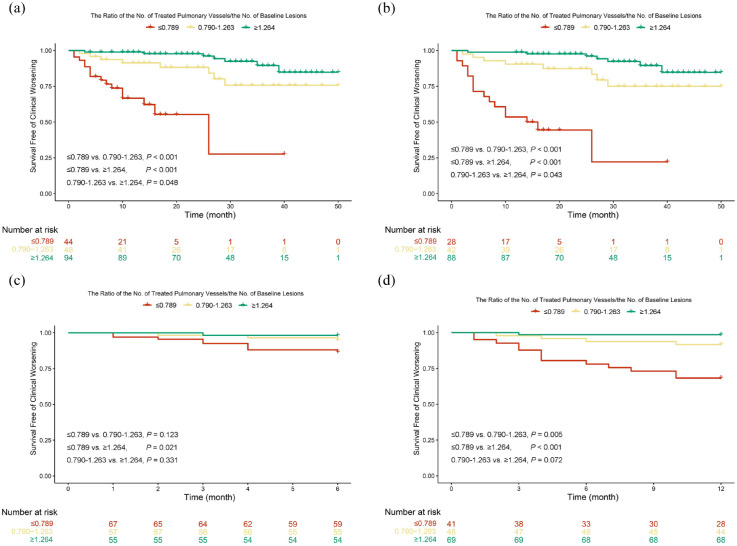
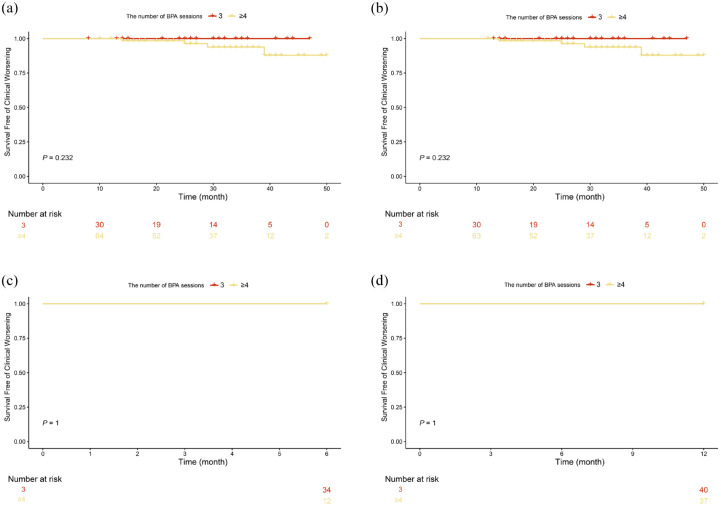
Results: After stratifying patients by the number of performed BPA sessions, most baseline parameters were comparable among groups. During follow-up, 31 (16.7%) of 186 patients experienced clinical worsening. The 6-month cumulative clinical worsening-free survival rates of ⩾2 performed sessions group were significantly higher than that of 1 performed session group. The 12-month cumulative rates of clinical worsening-free survival exhibited a declining pattern in the subsequent sequence: ⩾3, 2, and 1 performed BPA sessions, and this trend persisted when follow-up time exceeded 12 months. The 6-, 12-, and 24-month cumulative clinical worsening-free survival rates were comparable between patients with 3 and ⩾4 performed BPA sessions. Similar results were also observed when stratifying patients by the accumulative number of treated pulmonary vessels (⩽8, 9-16, ⩾17) and T/P (⩽0.789, 0.790-1.263, ⩾1.264).
Conclusion: To achieve optimal short-term outcomes, patients might need to undergo ⩾2 BPA sessions or have ⩾9 pulmonary vessels treated or have T/P ⩾0.790 within 6 months, and undergo ⩾3 BPA sessions or have ⩾17 pulmonary vessels treated or have T/P ⩾1.264 within 12 months.
Keywords: chronic thromboembolic pulmonary hypertension; interventional therapy; pulmonary hypertension; right heart failure.
Plain language summary
The least number of BPA session to reach a favorable outcomeWhy was the study done? Balloon pulmonary angioplasty (BPA) has been recommended for patients with chronic thromboembolic pulmonary hypertension, which can significantly improve patients’ hemodynamics. However, BPA is typically performed in a stepwise manner, and the duration from the initial session to the final session could extend over a year. If patients could not quickly undergo adequate number of BPA sessions and reach hemodynamic target due to various reasons, what is the best frequency of BPA for them? What did the researchers do? We retrospectively enrolled 186 BPA-treated patients diagnosed with chronic thromboembolic pulmonary hypertension. According to the accumulative number of BPA sessions, we divided patients into different groups to identify the best frequency of BPA to improve prognosis. What did the researchers find? Patients who received at least two BPA sessions within six months had significantly better prognosis than those with one BPA session. Patients who received at least three BPA sessions within a year had significantly better prognosis than those with two BPA sessions. What do the findings mean? To achieve optimal short-term outcome, patients might need to undergo at least two BPA sessions within six months, and undergo at least three BPA sessions within a year.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Figures
Similar articles
-
Predictors of early response to balloon pulmonary angioplasty in patients with inoperable chronic thromboembolic pulmonary hypertension.Ther Adv Respir Dis. 2022 Jan-Dec;16:17534666221138001. doi: 10.1177/17534666221138001. Ther Adv Respir Dis. 2022. PMID: 36411950 Free PMC article.
-
Improved hemodynamics and cardiopulmonary function in patients with inoperable chronic thromboembolic pulmonary hypertension after balloon pulmonary angioplasty.Respir Res. 2019 Nov 8;20(1):250. doi: 10.1186/s12931-019-1211-y. Respir Res. 2019. PMID: 31703589 Free PMC article.
-
Bilateral versus unilateral balloon pulmonary angioplasty for inoperable chronic thromboembolic pulmonary hypertension.Respir Res. 2022 May 7;23(1):117. doi: 10.1186/s12931-022-02017-6. Respir Res. 2022. PMID: 35525930 Free PMC article.
-
Balloon pulmonary angioplasty for chronic thromboembolic pulmonary hypertension: A systematic review.Respir Investig. 2018 Jul;56(4):332-341. doi: 10.1016/j.resinv.2018.03.004. Epub 2018 Jul 3. Respir Investig. 2018. PMID: 30008295
-
Balloon Pulmonary Angioplasty for Chronic Thromboembolic Pulmonary Hypertension.Cardiovasc Intervent Radiol. 2018 Dec;41(12):1826-1839. doi: 10.1007/s00270-018-2012-2. Epub 2018 Jul 23. Cardiovasc Intervent Radiol. 2018. PMID: 30039506 Review.
References
-
- Humbert M, Kovacs G, Hoeper MM, et al.. 2022 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Heart J 2022; 43: 3618–3731. - PubMed
-
- Zoppellaro G, Badawy MR, Squizzato A, et al.. Balloon pulmonary angioplasty in patients with chronic thromboembolic pulmonary hypertension – a systematic review and meta-analysis. Circ J 2019; 83: 1660–1667. - PubMed
-
- Kimura M, Kohno T, Kawakami T, et al.. Midterm effect of balloon pulmonary angioplasty on hemodynamics and subclinical myocardial damage in chronic thromboembolic pulmonary hypertension. Can J Cardiol 2017; 33: 463–470. - PubMed
-
- Aoki T, Sugimura K, Tatebe S, et al.. Comprehensive evaluation of the effectiveness and safety of balloon pulmonary angioplasty for inoperable chronic thrombo-embolic pulmonary hypertension: long-term effects and procedure-related complications. Eur Heart J 2017; 38: 3152–3159. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
