

Value of intravenous alteplase before thrombectomy among patients with tandem lesions and emergent carotid artery stenting: A subgroup analysis of the SWIFT DIRECT trial
- PMID: 38409874
- PMCID: PMC11235868
- DOI: 10.1111/ene.16256
Value of intravenous alteplase before thrombectomy among patients with tandem lesions and emergent carotid artery stenting: A subgroup analysis of the SWIFT DIRECT trial
Abstract
Background and purpose: The value of intravenous thrombolysis (IVT) in eligible tandem lesion patients undergoing endovascular treatment (EVT) is unknown. We investigated treatment effect heterogeneity of EVT + IVT versus EVT-only in tandem lesion patients. Additional analyses were performed for patients undergoing emergent internal carotid artery (ICA) stenting.
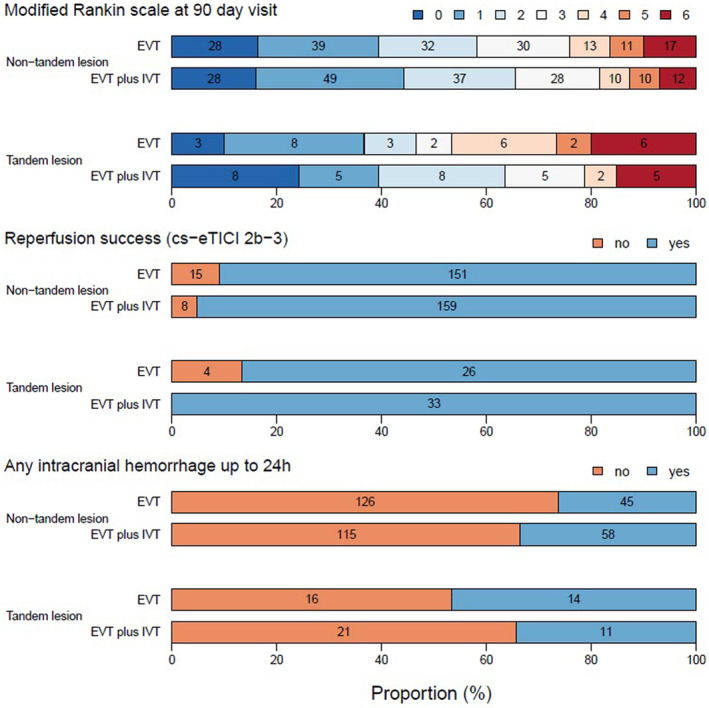
Methods: SWIFT DIRECT randomized IVT-eligible patients to either EVT + IVT or EVT-only. Primary outcome was 90-day functional independence (modified Rankin Scale score 0-2) after the index event. Secondary endpoints were reperfusion success, 24 h intracranial hemorrhage rate, and 90-day all-cause mortality. Interaction models were fitted for all predefined outcomes.
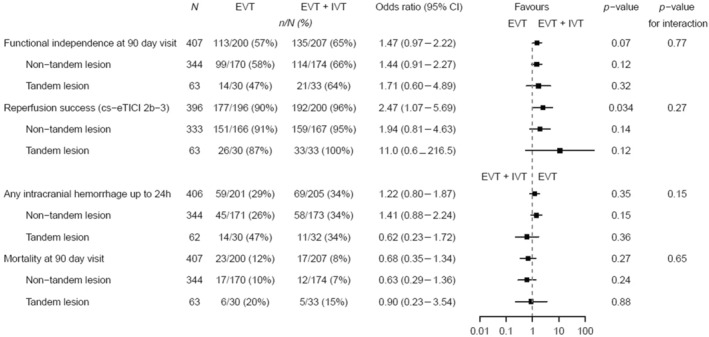
Results: Among 408 included patients, 63 (15.4%) had a tandem lesion and 33 (52.4%) received IVT. In patients with tandem lesions, 20 had undergone emergent ICA stenting (EVT + IVT: 9/33, 27.3%; EVT: 11/30, 36.7%). Tandem lesion did not show treatment effect modification of IVT on rates of functional independence (tandem lesion EVT + IVT vs. EVT: 63.6% vs. 46.7%, non-tandem lesion EVT + IVT vs. EVT: 65.6% vs. 58.2%; p for interaction = 0.77). IVT also did not increase the risk of intracranial hemorrhage among tandem lesion patients (tandem lesion EVT + IVT vs. EVT: 34.4% vs. 46.7%, non-tandem lesion EVT + IVT vs. EVT: 33.5% vs. 26.3%; p for interaction = 0.15). No heterogeneity was noted for other endpoints (p for interaction > 0.05).
Conclusions: No treatment effect heterogeneity of EVT + IVT versus EVT-only was observed among tandem lesion patients. Administering IVT in patients with anticipated emergent ICA stenting seems safe, and the latter should not be a factor to consider when deciding to administer IVT before EVT.
Keywords: extracranial stent; intravenous thrombolysis; mechanical thrombectomy; randomized controlled trial; tandem lesion.
© 2024 The Authors. European Journal of Neurology published by John Wiley & Sons Ltd on behalf of European Academy of Neurology.
Conflict of interest statement
T.D. reports paid consultancy work with Microvention outside the submitted work. D.J.S. reports grants from the Swiss National Science Foundation, Bangerter Rhyner Foundation, Swiss Heart Foundation, and AstraZeneca outside this study; and personal fees from Bayer, Alexion, BioXodes, and VarmX outside the submitted work. J.L. reports paid consultancy work with Medtronic, Stryker Neurovascular, and Microvention Europe outside the submitted work. E.I.P. reports grants from the Swiss National Science Foundation. U.F. reports financial support for the present study from Medtronic; research grants from the Medtronic BEYOND SWIFT registry, the Swiss National Science Foundation, and the Swiss Heart Foundation; and consulting fees from Medtronic, Stryker, and CSL Behring (fees paid to institution). J.K. reports financial support from Medtronic for the BEYOND SWIFT registry (fees paid to institution), and research grants from the Swiss National Science Foundation supporting the TECNO trial (fees paid to institution), Swiss Academy of Medical Sciences supporting MRI research (fees paid to institution), and Swiss Heart Foundation supporting cardiac MRI in the etiological workup of stroke patients (fees paid to institution). None of the other authors has any conflict of interest to disclose.
Figures
Similar articles
-
Endovascular therapy with or without intravenous thrombolysis in acute stroke with tandem occlusion.J Neurointerv Surg. 2022 Apr;14(4):314-320. doi: 10.1136/neurintsurg-2020-017202. Epub 2021 Apr 28. J Neurointerv Surg. 2022. PMID: 33911016
-
Cost-effectiveness of thrombectomy alone versus alteplase before thrombectomy in acute ischemic stroke: results from the DIRECT-MT.J Neurosurg. 2023 Feb 10;139(3):678-686. doi: 10.3171/2022.12.JNS221791. Print 2023 Sep 1. J Neurosurg. 2023. PMID: 36790013 Clinical Trial.
-
Effect of Intravenous Alteplase Treatment on First-Line Stent Retriever Versus Aspiration Alone During Endovascular Treatment.Stroke. 2022 Nov;53(11):3278-3288. doi: 10.1161/STROKEAHA.121.038390. Epub 2022 Jul 25. Stroke. 2022. PMID: 35876018 Clinical Trial.
-
Bridging versus Direct Mechanical Thrombectomy in Acute Ischemic Stroke: A Subgroup Pooled Meta-Analysis for Time of Intervention, Eligibility, and Study Design.Cerebrovasc Dis. 2020;49(2):223-232. doi: 10.1159/000507844. Epub 2020 Apr 24. Cerebrovasc Dis. 2020. PMID: 32335550
-
Acute Ischemic Stroke Therapy in Infective Endocarditis: Case Series and Systematic Review.J Stroke Cerebrovasc Dis. 2019 Aug;28(8):2207-2212. doi: 10.1016/j.jstrokecerebrovasdis.2019.04.039. Epub 2019 May 23. J Stroke Cerebrovasc Dis. 2019. PMID: 31129109
Cited by
-
Endovascular management of tandem occlusions: current evidence and future directions.J Neurointerv Surg. 2025 Aug 7:jnis-2025-023793. doi: 10.1136/jnis-2025-023793. Online ahead of print. J Neurointerv Surg. 2025. PMID: 40780815 Free PMC article. Review.
References
-
- Papanagiotou P, Haussen DC, Turjman F, et al. Carotid stenting with antithrombotic agents and intracranial thrombectomy leads to the highest recanalization rate in patients with acute stroke with tandem lesions. JACC Cardiovasc Interv. 2018;11(13):1290‐1299. doi:10.1016/j.jcin.2018.05.036 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
