

Stapled Anastomosis Versus Hand-Sewn Anastomosis With Mucosectomy for Ileal Pouch-Anal Anastomosis: A Systematic Review and Meta-analysis of Postoperative Outcomes, Functional Outcomes, and Oncological Safety
- PMID: 38410083
- PMCID: PMC10898296
- DOI: 10.1177/10732748241236338
Stapled Anastomosis Versus Hand-Sewn Anastomosis With Mucosectomy for Ileal Pouch-Anal Anastomosis: A Systematic Review and Meta-analysis of Postoperative Outcomes, Functional Outcomes, and Oncological Safety
Abstract
Purpose: This systematic review and meta-analysis aimed to compare outcomes between stapled ileal pouch-anal anastomosis (IPAA) and hand-sewn IPAA with mucosectomy in cases of ulcerative colitis and familial adenomatous polyposis.
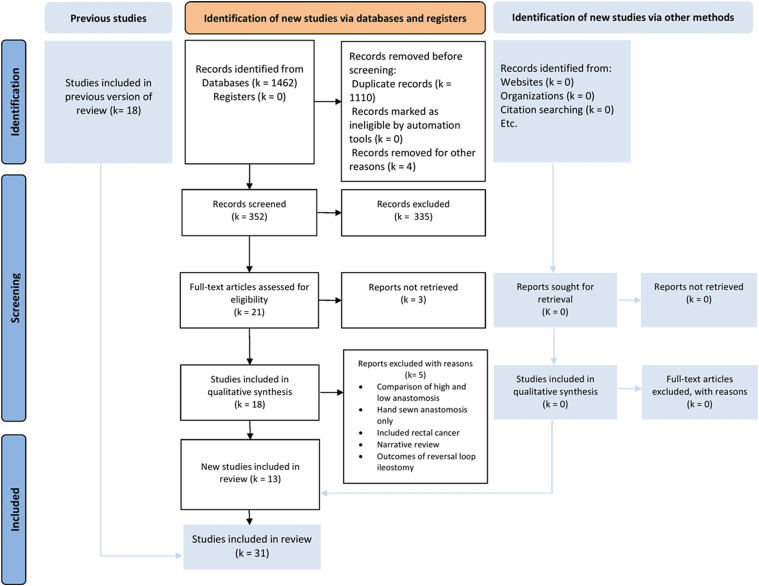
Methods: This systematic review and meta-analysis was performed according to the Preferred Reporting Items for Systematic Review and Meta-analysis) guidelines 2020 and AMSTAR 2 (Assessing the methodological quality of systematic reviews) guidelines. We included randomized clinical trials (RCTs) and controlled clinical trials (CCTs). Subgroup analysis was performed according to the indication for surgery.
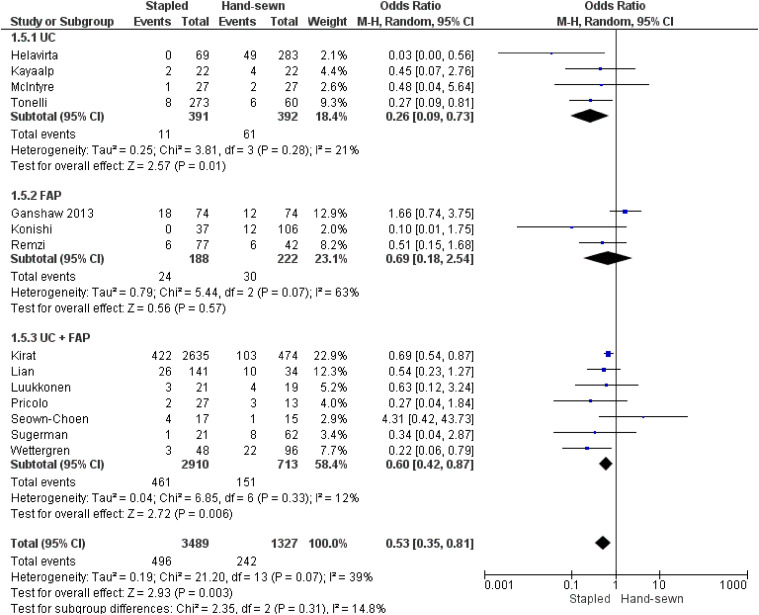
Results: The bibliographic research yielded 31 trials: 3 RCTs, 5 prospective clinical trials, and 24 CCTs including 8872 patients: 4871 patients in the stapled group and 4038 in the hand-sewn group. Regarding postoperative outcomes, the stapled group had a lower rate of anastomotic stricture, small bowel obstruction, and ileal pouch failure. There were no differences between the 2 groups in terms of operative time, anastomotic leak, pelvic sepsis, pouchitis, or hospital stay. For functional outcomes, the stapled group was associated with greater outcomes in terms of seepage per day and by night, pad use, night incontinence, resting pressure, and squeeze pressure. There were no differences in stool Frequency per 24h, stool frequency at night, antidiarrheal medication, sexual impotence, or length of the high-pressure zone. There was no difference between the 2 groups in terms of dysplasia and neoplasia.
Conclusions: Compared to hand-sewn anastomosis, stapled ileoanal anastomosis leads to a large reduction in anastomotic stricture, small bowel obstruction, ileal pouch failure, seepage by day and night, pad use, and night incontinence. This may ensure a higher resting pressure and squeeze pressure in manometry evaluation.
Protocol registration: The protocol was registered at PROSPERO under CRD 42022379880.
Keywords: functional results; hand-sewn anastomosis; ileal pouch-anal anastomosis; oncological outcomes; postoperative outcomes; stapled anastomosis.
Conflict of interest statement
Declaration of Conflicting InterestsThe author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Page MJ, McKenzie JE, Bossuyt PM, et al. Updating guidance for reporting systematic reviews: development of the PRISMA 2020 statement. J Clin Epidemiol. 2021;134:103-112. - PubMed
-
- Slim K, Nini E, Forestier D, Kwiatkowski F, Panis Y, Chipponi J. Methodological index for non-randomized studies (MINORS): development and validation of a new instrument. ANZ J Surg. 2003;73(9):712-716. - PubMed
-
- Yang ZR, Sun F, Zhan SY. Risk on bias assessment:(2) Revised Cochrane risk of bias tool for individually randomized, parallel group trials (RoB2. 0). Zhonghua Liu Xing Bing Xue Za Zhi Zhonghua Liuxingbingxue Zazhi. 2017;38(9):1285-1291. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
